Summary
This review discusses echocardiographic evaluation in mechanically ventilated (MV) patients, highlighting the complex heart–lung interactions influenced by positive pressure ventilation, especially focusing on the right ventricle (RV). Echocardiography serves as a crucial bedside tool to assess RV dimensions, function, and response to mechanical ventilation. Given the challenges in assessing fluid responsiveness and diaphragmatic function in these patients, dynamic methods such as the passive leg raise, fluid challenge, and end-expiration occlusion test are preferred. Diaphragmatic ultrasound is emphasized for identifying complications, guiding ventilatory management, and improving prognostication during weaning.

Key Points
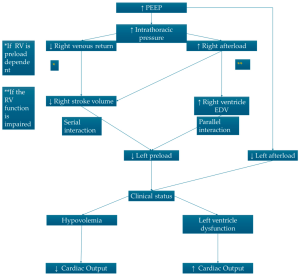
- Heart–Lung Interaction: Mechanical ventilation with positive end-expiratory pressure (PEEP) significantly impacts heart function, particularly the right ventricle, by altering intrathoracic pressures and consequently affecting venous return and cardiac output.
- Right Ventricular Assessment: Echocardiographic evaluation of RV dimensions, wall thickness, interventricular septum position, fractional area change (FAC), tricuspid annular plane systolic excursion (TAPSE), and pulmonary artery pressures are essential, given the RV’s susceptibility to increased intrathoracic pressures.
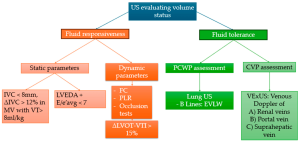
- Fluid Responsiveness Evaluation: In mechanically ventilated patients, static measurements (such as inferior vena cava diameter) are often unreliable, making dynamic tests including passive leg raise (PLR), fluid challenge (FC), and end-expiration occlusion (EEO) more appropriate for accurate assessment.
- Diaphragm Function and Dysfunction: Diaphragmatic ultrasound helps in early detection and monitoring of ventilator-induced diaphragmatic dysfunction (VIDD). This includes measurement of diaphragmatic thickness, thickening fraction, and movement amplitude, crucial for weaning decisions.
- Left Ventricular Filling Pressure: Echocardiographic assessment of left atrial pressure (LAP) is useful for managing ventilatory settings, particularly to understand preload conditions; however, caution is required as increased pericardial pressures during mechanical ventilation can confound interpretations.
- Interventricular Septal Shift: Mechanical ventilation, particularly at high pressures, can cause a paradoxical interventricular septal shift toward the left ventricle, leading to altered cardiac mechanics, decreased cardiac output, and compromised hemodynamics.
- Assessment of Venous Congestion: Ultrasound evaluation of central and peripheral venous structures, including inferior vena cava (IVC) and internal jugular vein (IJV) distensibility indices, provides non-invasive insights into fluid overload and systemic congestion status in ventilated patients.
- Dynamic Echocardiographic Tests: The article emphasizes dynamic tests like the passive leg raise, fluid challenge, and respiratory cycle-based occlusion tests as superior methods for evaluating preload responsiveness compared to static measures, especially under lung-protective ventilation strategies.
- Clinical Implications for Echocardiography: Echocardiography is invaluable for guiding the management of mechanically ventilated patients, allowing clinicians to tailor ventilator settings, fluid administration, and interventions based on real-time hemodynamic and respiratory data.
- Future Directions: The authors advocate for routine integration of echocardiographic protocols in ICU practices, promoting a multidisciplinary approach and enhancing patient outcomes through better-informed clinical decisions and tailored therapies.
Conclusion
Echocardiography represents a cornerstone in managing mechanically ventilated patients, providing comprehensive, non-invasive evaluation of cardiac function, fluid responsiveness, and diaphragmatic status. Its use facilitates better clinical decision-making, improved patient management, and optimization of outcomes, particularly in critically ill populations.
Discussion Questions
- How can echocardiographic assessments be more systematically integrated into standard ICU care to optimize ventilatory management and prevent ventilator-induced cardiac dysfunction?
- Given the complexity of interpreting echocardiographic findings in mechanically ventilated patients, what standardized training or educational initiatives could enhance clinician proficiency?
- In clinical practice, what are the main challenges or barriers to implementing routine diaphragmatic ultrasound monitoring, and how might these be overcome?
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.

