Summary
This prospective cohort study evaluated the utility of serial point-of-care ultrasound (POCUS) during cardiopulmonary resuscitation (CPR) to determine optimal timing for terminating resuscitation efforts in patients presenting with non-shockable cardiac arrest rhythms. Conducted in two academic hospitals, serial ultrasounds every two minutes were used to measure cardiac standstill duration and predict return of spontaneous circulation (ROSC). Results showed that cardiac standstill lasting ≥10 minutes was 100% predictive of failure to achieve ROSC, indicating that serial POCUS provides robust prognostic guidance, potentially aiding critical clinical decision-making during cardiac arrest management.
Key Points
- Background and Clinical Challenge: Determining when to terminate CPR in patients with cardiac arrest and non-shockable rhythms (asystole or pulseless electrical activity [PEA]) is clinically challenging due to uncertain prognostic indicators and ethical considerations.
- Study Objective and Design: This prospective cohort study aimed to validate serial POCUS as a real-time, reliable tool to predict resuscitation futility based on cardiac standstill duration in adults experiencing non-traumatic cardiac arrest.
- Serial POCUS Methodology: Cardiac ultrasound assessments were performed every two minutes during ongoing CPR, with cardiac standstill defined as absence of any visible cardiac activity, allowing longitudinal tracking of cardiac function.
- Study Population and Setting: Conducted between June 2024 and March 2025, the study enrolled 154 adult patients from two academic hospitals who suffered either out-of-hospital cardiac arrest (OHCA, 81.8%) or in-hospital cardiac arrest (IHCA, 18.2%).
- Primary Outcomes and Survival Rates: ROSC was achieved in 24.7% of patients, while only 5.8% survived to hospital discharge. Initial cardiac activity detected on ultrasound significantly predicted ROSC (52.1% vs. 12.3% without activity, p < 0.001) and survival (16.7% vs. 0.69%, p < 0.001).
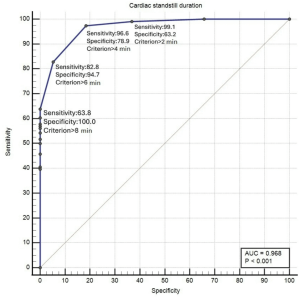
- Cardiac Standstill as Prognostic Indicator: Cardiac standstill duration strongly correlated with resuscitation outcomes. Patients exhibiting continuous cardiac standstill ≥10 minutes showed a 100% positive predictive value for non-ROSC, suggesting robust specificity in predicting futile resuscitation.
- Comparison of Arrest Types: Patients with IHCA had significantly higher ROSC rates (50%) compared to OHCA (19%), indicating the influence of immediate availability of advanced resuscitation resources.
- Integration into Clinical Practice: The authors advocate the routine incorporation of serial POCUS into resuscitation algorithms, emphasizing its role in optimizing clinical decision-making and resource allocation, particularly in emergency departments.
- Limitations and Considerations: Despite high predictive accuracy, limitations included potential selection bias, limited generalizability due to the study’s single-region design, and challenges in consistently blinding the clinical team to ultrasound findings.
- Recommendations for Future Research: Further larger-scale studies are needed to validate these findings broadly, refine cardiac standstill thresholds, and establish definitive guidelines for integrating serial POCUS into resuscitation termination protocols.
Conclusion
Serial POCUS provides significant predictive value for guiding termination of resuscitation in non-shockable cardiac arrest. Persistent cardiac standstill of 10 minutes or longer consistently predicts failure to achieve ROSC, suggesting that serial ultrasound assessments should be systematically integrated into advanced resuscitation protocols to enhance clinical decision-making and optimize resource utilization.

Discussion Questions
- How can clinical teams effectively integrate serial POCUS protocols into existing cardiac arrest guidelines to enhance decision-making without disrupting standard CPR processes?
- What training and infrastructure are necessary to ensure widespread adoption and standardization of serial ultrasound use during cardiac arrests in diverse healthcare settings?
- Given ethical considerations surrounding CPR termination, how can clinicians best communicate serial POCUS findings to family members or legal representatives to facilitate understanding and shared decision-making?
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.