Summary
This article explores the use of electrical impedance tomography (EIT) for assessing pulmonary perfusion in critically ill pediatric patients with congenital heart disease (CHD). The study demonstrates the reliability and accuracy of EIT, a non-invasive, real-time, bedside, and radiation-free technique, through three complex clinical cases. The results from EIT were consistent with those obtained using traditional imaging modalities like CT, MRI, and angiography, validating its potential utility in monitoring pulmonary perfusion and guiding clinical decisions in this challenging patient population.

Key Points
- Clinical Need for Improved Perfusion Assessment: Evaluating pulmonary perfusion in pediatric CHD patients is complicated due to anatomical variations affecting blood flow, highlighting the need for accurate bedside diagnostic tools.
- Electrical Impedance Tomography (EIT) Methodology: EIT assesses regional lung ventilation and perfusion by detecting impedance changes, particularly during the injection of a hypertonic saline bolus (0.5 ml/kg of 5% saline), offering real-time, radiation-free imaging at the bedside.
- Validation of EIT Against Traditional Imaging Techniques: EIT perfusion assessments correlated well with findings from established imaging techniques such as computed tomography (CT), magnetic resonance imaging (MRI), and angiography, confirming its reliability.
- Case 1 – Postoperative TGA Patient: In a newborn post arterial-switch operation for transposition of the great arteries (TGA), EIT identified normal lung perfusion and ventilation–perfusion matching, aligning with echocardiographic findings and supporting clinical management.
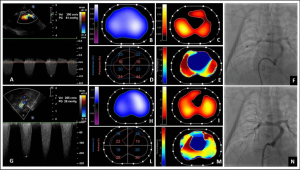
- Case 2 – Tetralogy of Fallot (TOF) with Pulmonary Branch Stenosis: An infant with severe hypoxemia following TOF repair demonstrated through EIT significant reduction in left lung perfusion due to pulmonary artery stenosis, effectively guiding treatment decisions when traditional therapies failed.
- Case 3 – Hypoxemia After Norwood–Sano Procedure: In an infant with a univentricular heart repair (Norwood–Sano), EIT precisely identified perfusion impairment caused by Sano conduit stenosis, facilitating targeted interventions, including stent placement, and monitoring improvements post-intervention.
- Ventilation–Perfusion Matching Insights: EIT allowed detailed, pixel-level analysis of ventilation-perfusion relationships, crucial for understanding physiological disturbances, identifying mismatched areas, and tailoring individualized respiratory and cardiovascular therapies.
- Advantages Over Conventional Methods: EIT’s bedside availability, continuous monitoring capability, and radiation-free nature represent significant clinical advantages over conventional imaging, especially relevant for critically ill pediatric patients.
- Future Clinical Implementation and Standardization: While this series confirms EIT’s feasibility and clinical value, further research is essential to standardize protocols, refine analysis techniques, and validate broader clinical utility across various pediatric CHD populations.
- Potential Clinical Impact and Outcomes: Routine adoption of EIT in pediatric critical care for CHD patients could significantly enhance bedside diagnostic precision, improve targeted therapeutic strategies, reduce reliance on invasive and resource-intensive procedures, and ultimately improve patient outcomes.

Conclusion
Electrical impedance tomography offers a novel, effective, and safe bedside tool for real-time, non-invasive pulmonary perfusion monitoring in pediatric patients with complex congenital heart disease. Demonstrating accuracy comparable to traditional imaging techniques, EIT has significant potential to improve clinical management, inform targeted therapeutic interventions, and optimize patient outcomes.
Discussion Questions
- How can institutions effectively implement standardized EIT protocols into routine pediatric ICU care, ensuring reliability and consistency across diverse clinical scenarios?
- What research is required to fully establish EIT’s diagnostic accuracy and predictive value compared to current gold-standard imaging methods in pediatric congenital heart disease?
- Given EIT’s unique benefits and challenges, what practical strategies can help facilitate its widespread clinical adoption in resource-limited healthcare settings?
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.

