Abstract
Sepsis, one of the leading causes of ICU mortality worldwide, remains a diagnostic and therapeutic challenge due to its nonspecific presentation and rapidly evolving course. In this narrative review, Tocu and colleagues explore the emerging role of artificial intelligence (AI) in diagnosing and predicting sepsis. Drawing from 45 studies between 2016 and 2024, the review highlights the performance of machine learning (ML) and deep learning (DL) algorithms—many achieving AUC values above 0.90—for early recognition and mortality prediction. AI tools like TREWS and InSight have demonstrated real-world success in reducing time to treatment and mortality. However, persistent barriers include limited transparency, inconsistent data quality, and the need for multicenter validation before widespread adoption.
Key Insights:
1️⃣ Sepsis: A Race Against Time Sepsis causes over 11 million deaths annually, with mortality rising sharply when recognition is delayed. Early diagnosis and targeted intervention remain essential—yet existing tools like qSOFA and SIRS lack precision, creating an urgent demand for AI-driven early warning systems.
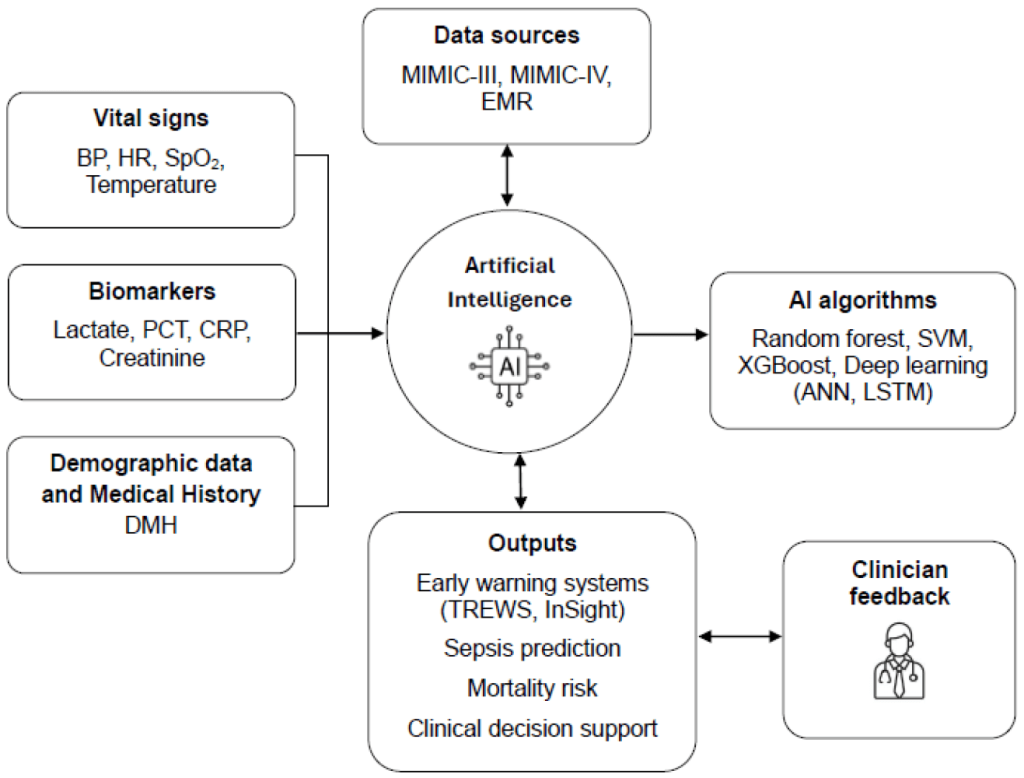
2️⃣ The Rise of AI in Sepsis Care: AI enables the real-time analysis of complex, multidimensional data—vital signs, labs, and EHR trends—identifying subtle physiological deterioration far earlier than clinical scoring systems can. Unlike static tools, AI models continuously adapt to the evolving patient trajectory.
3️⃣ Landmark Algorithms and Systems: Among the most validated systems, TREWS (Johns Hopkins) and InSight (Dascena) have achieved clinical deployment. TREWS reduced antibiotic administration time by 1.85 hours and lowered mortality by 18.2%, while InSight attained AUCs of 0.93 (sepsis) and 0.90 (shock), outperforming all traditional scores.
4️⃣ Deep Learning and Temporal Models: Recurrent neural networks (RNNs) and long short-term memory (LSTM) architectures excel in capturing dynamic trends in vital signs and labs. These models can anticipate sepsis onset 4–12 hours before clinical recognition, enabling earlier clinical response and potentially saving lives.
5️⃣ Predictive Power of Big Data: Databases like MIMIC-IV and eICU-CRD underpin most AI studies, housing millions of ICU data points. Models trained on these datasets achieved predictive accuracies of 84–94%, confirming AI’s capacity to generalize patterns across populations—though issues of bias and data completeness persist.
6️⃣ Beyond Prediction—Personalized Medicine: The review envisions the integration of “digital twins”—virtual patient simulations that mirror individual physiology to personalize therapy, from fluid resuscitation to ventilator settings. This approach aligns AI with the broader trend toward precision medicine.
7️⃣ Ethical and Interpretability Challenges: “Black box” models hinder clinician trust. Despite innovations like SHAP and LIME to explain predictions, interpretability remains limited. Ethical questions around liability, privacy (GDPR/HIPAA), and algorithmic bias must be addressed before AI becomes standard in ICU workflows.
8️⃣ Workflow Integration and Human–AI Collaboration: AI should complement—not replace—clinicians. Integration into EMR systems and training staff to interpret AI outputs are key to success. Over-alerting and “data fatigue” remain major risks, underscoring the need for balanced alert thresholds and contextualized risk visualization.
9️⃣ The Evidence Gap: While performance metrics are promising, most models lack external or prospective validation. Few have been tested through randomized controlled trials (RCTs). Standardized sepsis labeling (Sepsis-3) and multicenter validation are necessary next steps for regulatory approval.
🔟 The Road Ahead: Explainable and Federated AI Future sepsis AI will rely on federated learning (cross-hospital model training without centralizing data), explainable algorithms, and integrative dashboards displaying the clinical reasoning behind alerts. These innovations aim to ensure scalability, safety, and clinician confidence.
🧩 Clinical Takeaways
- AI now surpasses classical scores (SOFA, qSOFA, SIRS) in both accuracy and lead time.
- Prospective systems like TREWS demonstrate real-world mortality benefits.
- True integration requires transparent algorithms, clinician education, and ethical governance.
- The next frontier is real-time, interpretable, and adaptive AI—supporting rather than replacing the clinician’s judgment.
🗣️ Discussion
Can AI-driven sepsis prediction truly reduce mortality without overwhelming clinicians—or will overreliance on algorithms risk clinical intuition and patient individuality?

