1. Why This Study Matters — Why You Should Read This
Physiology at the bedside is often guesswork. We titrate PEEP. We adjust driving pressure. We interpret compliance as a global signal, even though ARDS is intensely regional.
But imagine if we had a patient-specific digital model — a “virtual twin” — that could simulate regional lung mechanics, predict strain, and help us choose ventilator settings based on physics, not approximation.
This article validates exactly that concept.
This could become one of the most important technological advances in ARDS management since the introduction of low tidal volume ventilation.
2. The Study in 5 Lines
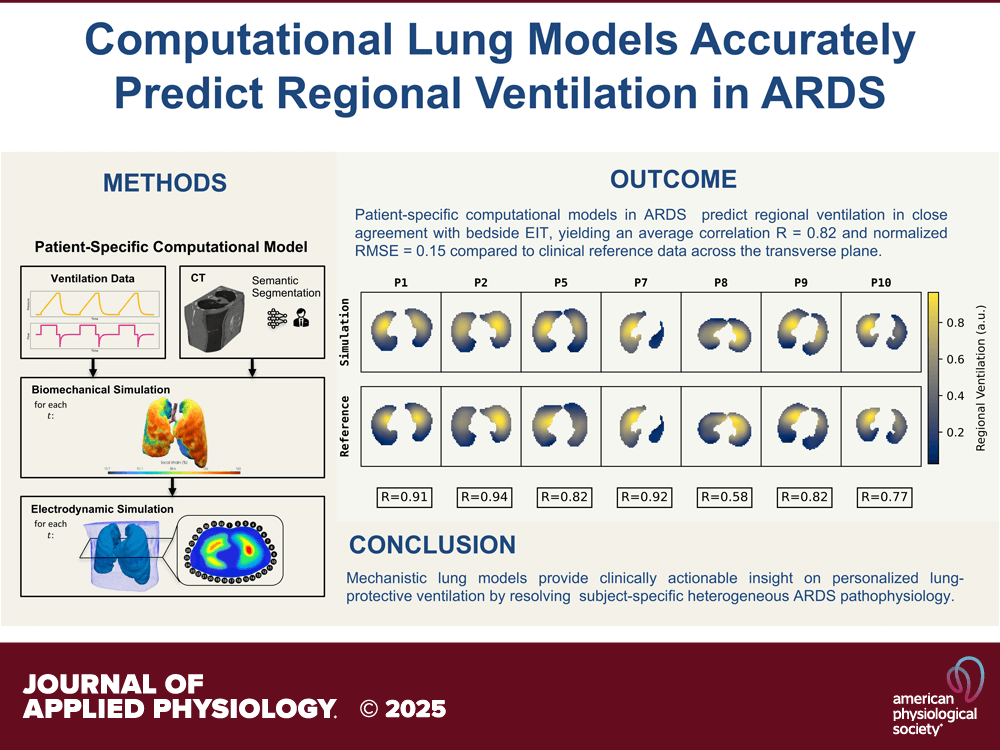
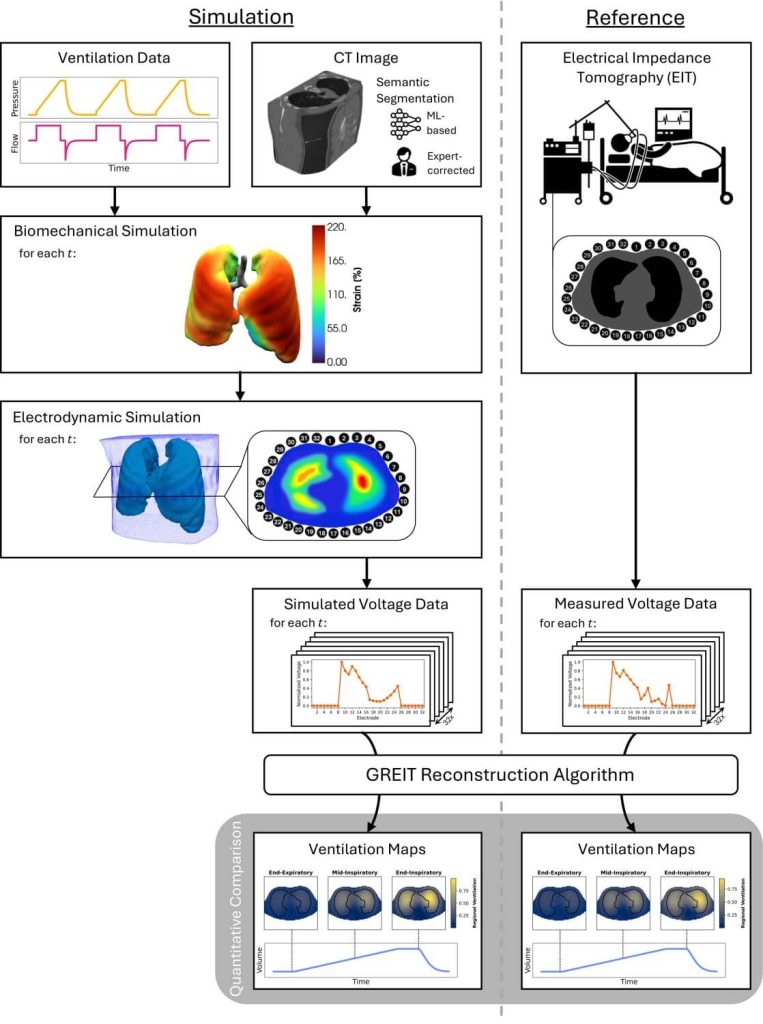
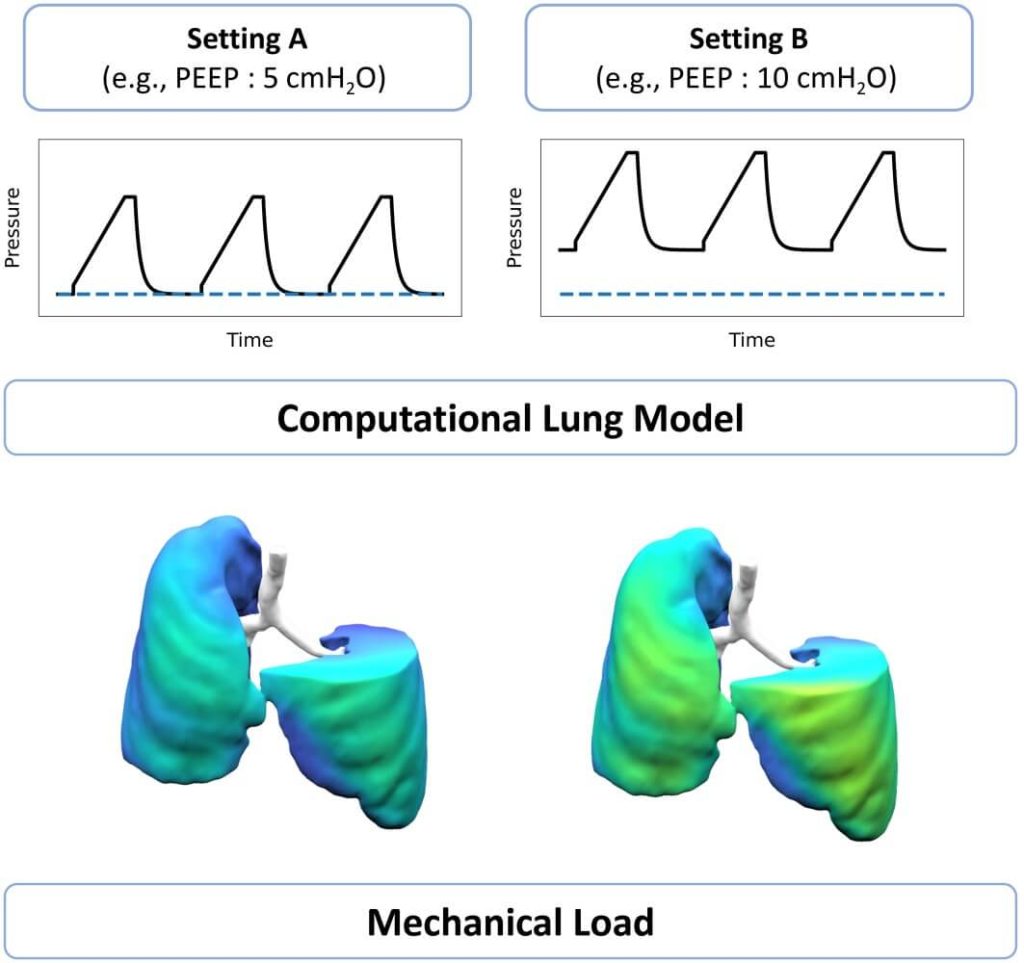
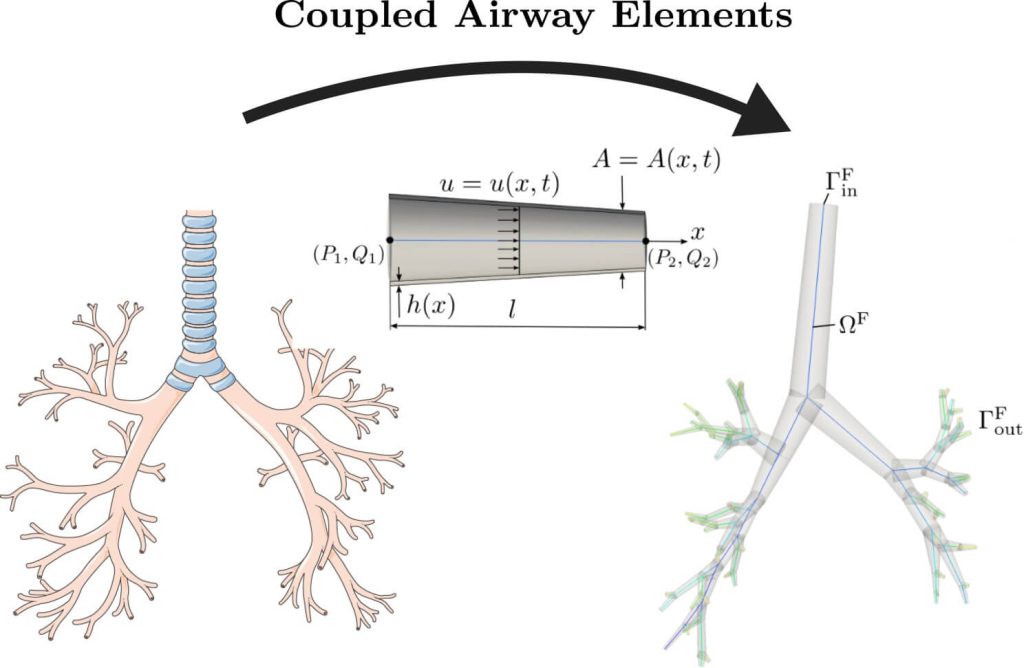
- Researchers built a physics-based, patient-specific lung model using CT-derived geometry and nonlinear tissue mechanics.
- They tested whether the model could predict regional ventilation and tidal strain under clinically used ventilator settings.
- Predictions were compared with EIT measurements in mechanically ventilated ARDS patients.
- The model showed strong agreement with EIT across multiple PEEP levels.
- This supports the future use of digital twins to optimize ventilation and prevent VILI through individualized simulation.
3. What They Actually Found — The Clinically Important Insights
1️⃣ The physics-based digital twin accurately predicted regional lung behavior
Across PEEP steps, the model reliably predicted:
- regional tidal volume distribution
- impedance changes
- recruitment patterns
Correlation with EIT was consistently strong, especially in dependent regions — where VILI risk is highest.
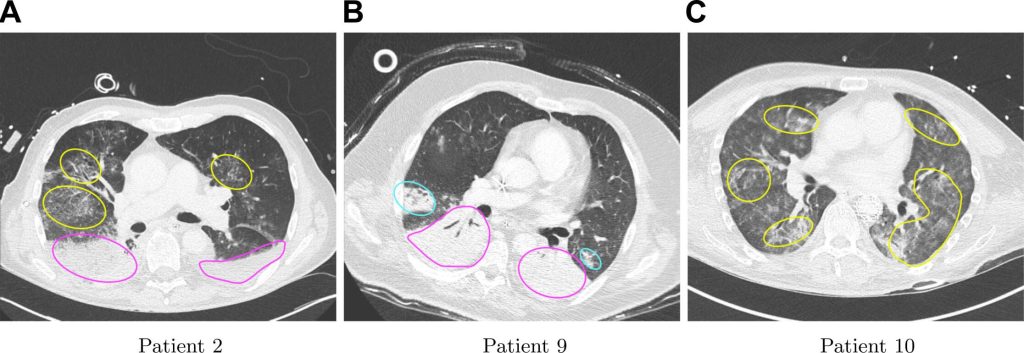
2️⃣ The model captured heterogeneity — the central problem in ARDS
ARDS is not a uniform disease. Some units are collapsed, some overdistended, some normal. The digital twin mirrored this heterogeneity, identifying regions with:
- high local strain
- limited recruitability
- risk of overdistension
This is something no single ventilator variable (like compliance or driving pressure) can fully capture.
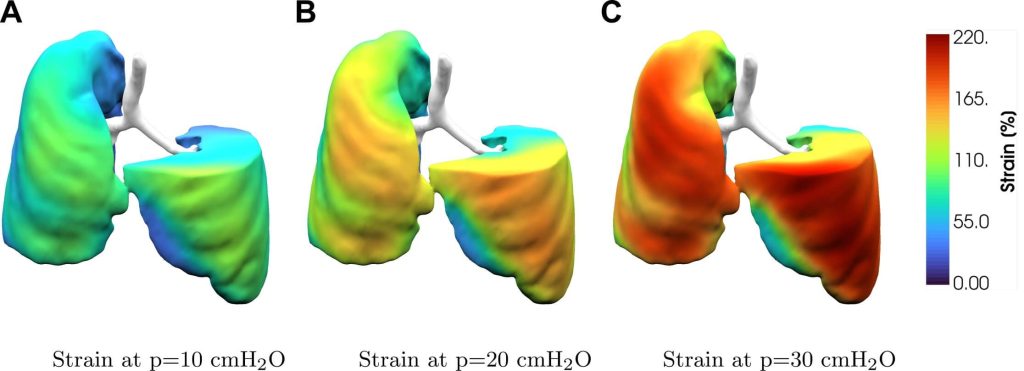
3️⃣ It predicted how individual lungs respond to PEEP — with remarkable accuracy
A key finding: The model predicted which regions would recruit and which would not at higher PEEP.
This is essential because PEEP is beneficial only when it recruits unstable units — not when it overinflates already open tissue.
The model allows clinicians to simulate this before applying PEEP in real life.
4️⃣ The digital twin could identify patients at risk of VILI before it happens
By computing regional strain, the model offers a way to anticipate:
- overdistension
- pendelluft
- excessive transpulmonary stress
- strain gradients that drive injury
This could eventually allow preventative ventilation — instead of reactive settings based on deterioration.
5️⃣ Even with simplified assumptions, predictions remained robust
Despite having to estimate some parameters (e.g., tissue stiffness, boundary conditions), the model still performed well. This proves its clinical resilience — a crucial step toward real-world adoption.
6️⃣ It outperformed traditional metrics in explaining patient variability
Global compliance or oxygenation tell only part of the story. Regional strain maps from the model explained why patients with similar global metrics behave differently on PEEP trials.
7️⃣ This approach could revolutionize PEEP titration
Instead of escalating pressure and “seeing what happens,” clinicians could simulate:
- the optimal PEEP for recruitment
- the point where overdistension begins
- how changes in driving pressure redistribute strain
This could redefine lung-protective ventilation.
8️⃣ The model aligns with EIT but provides deeper granularity
EIT shows global quadrant-level ventilation. The digital twin offers voxel-level mechanics with physics-based interpretation.
EIT is valuable — but this model provides a high-fidelity mechanical explanation for what EIT visualizes.
9️⃣ This is a validation step — not yet ready for bedside plug-and-play
The authors emphasize that while performance was strong, future versions require:
- real-time computation
- automated parameter fitting
- bedside integration
- larger prospective trials
🔟 The future: a bedside mechanical simulation for every ARDS patient
If validated in large cohorts, digital twins could allow clinicians to:
- test ventilator strategies
- predict strain distribution
- simulate prone positioning
- forecast recruitment
- guide personalized ventilation
This could be as disruptive to critical care as EIT, ECMO, or the ARDSNet trial.
4. How This Should Influence Your Practice
- Start thinking regionally, not globally. ARDS is a disease of spatial heterogeneity; digital models expose that reality.
- Recognize that PEEP cannot be one-size-fits-all. This study reinforces that optimal PEEP varies dramatically by patient and region.
- Support innovation that brings physics to the bedside. This research validates a credible pathway toward precision ventilation.
- Prepare for a future where we simulate before we ventilate. ICU mechanical ventilation may shift from empiric titration to computational prediction.
5. Bottom Line for Clinicians
Digital twins may become the next major advance in ARDS management — enabling individualized prediction of regional mechanics, strain, and PEEP responsiveness.
This study successfully validates the concept, showing strong agreement with EIT and a powerful ability to map heterogeneity at high resolution. It marks a serious step toward true personalized ventilation.
6. A Question for Our Readers
If you could simulate regional strain and recruitment before adjusting the ventilator, would you rely on a physics-based model to guide PEEP titration in ARDS?
Why or why not?
Your thoughts will help shape future ICCN community discussions.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

