Why This Study Matters — Why You Should Read This
Obesity. Abdominal compartment syndrome. Massive chest wall load. We see these patients every day. We crank up PEEP, perform recruitment maneuvers, increase pressures…and yet the lung refuses to open.
So what if the problem isn’t pressure at all? What if the missing variable is time?
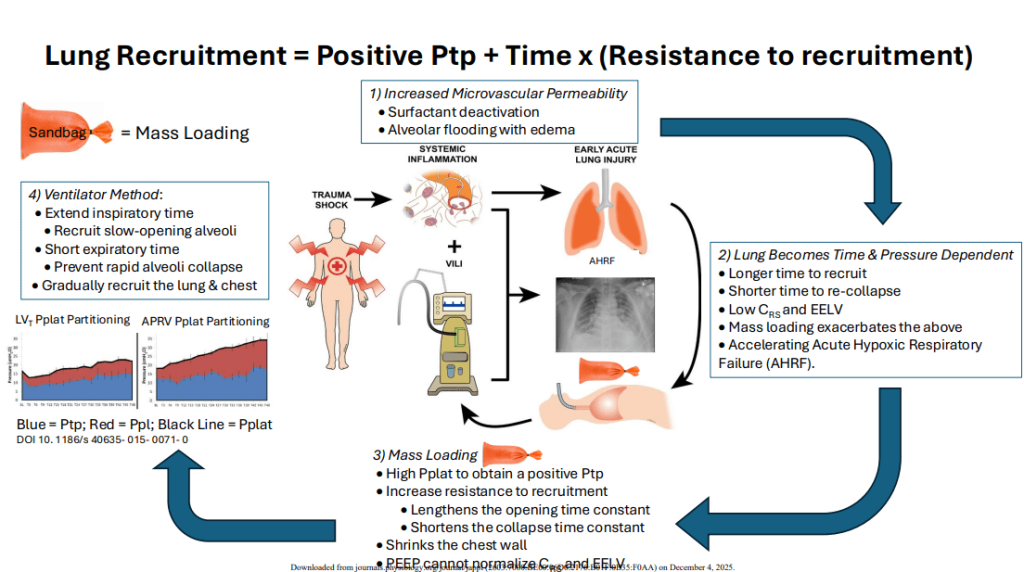
This commentary by Nieman, Araos, Habashi, and colleagues builds a compelling physiologic argument: Mass-loaded lungs don’t just need more pressure — they need more time to reopen and less time to collapse.
This paper reframes one of the most difficult clinical challenges in ARDS and AHRF: how to ventilate patients whose chest wall is literally working against them.
2. The Study in 5 Lines
- Experimental models show that any increase in external mass (obesity, ACS, chest wall weight) decreases lung volume and accelerates collapse.
- PEEP alone fails to recruit these lungs because their opening time constants are too long for conventional inspiratory time.
- AHRF creates a nonlinear time–pressure environment where alveoli collapse quickly but open very slowly.
- Mass loading amplifies this mismatch, increasing VILI risk and making traditional low Vt ventilation insufficient.
- The authors propose using ventilator time manipulation — long inspiratory times and short expiratory times — to counter mass loading and gradually restore FRC.
3. What They Actually Found — The Clinically Important Insights
1️⃣ Mass loading reduces FRC even when “optimal” PEEP is applied
The Nova pig study demonstrated that simply adding weight to the thorax and abdomen reduces EELV and worsens compliance. PEEP failed to restore lung volume because the alveoli required longer opening time constants than conventional breathing allowed.
2️⃣ In AHRF, the lung becomes both pressure- AND time-dependent
AHRF lungs:
- take more time to open
- collapse faster
- show severe heterogeneity
- experience higher shear stress
Figure 1 in the article visualizes this perfectly — recruitment slows while de-recruitment speeds up.
This is the physiology of why VILI becomes self-perpetuating in these patients.
3️⃣ PEEP alone cannot overcome high pleural pressures
Mass loading raises pleural pressure so much that external PEEP simply can’t create adequate transpulmonary pressure, even at high levels.
More pressure is not the solution — more time is.
4️⃣ Slow-opening alveoli require sustained inspiratory pressure to achieve recruitment
Opening pressure is only part of the story. Certain alveoli need time under tension to overcome viscoelastic resistance and fully recruit.
Short inspiratory times = failure to recruit. Conventional ventilation simply can’t give these units enough time.
5️⃣ Collapse occurs rapidly when expiratory time is too long
Conversely, mass-loaded lungs collapse extremely fast when given enough time to exhale. This explains why these patients:
- de-recruit between breaths
- have poor compliance
- require escalating pressures
- develop worsening VILI
You cannot “out-PEEP” this collapse mechanism.
6️⃣ The answer is a time-based strategy: prolong inspiration, shorten expiration
Nieman et al. describe the physiology behind applying:
- long inspiratory times (for recruitment)
- short expiratory times (to prevent collapse)
This dual effect gradually “ratchets open” the lung. It explains why APRV/TCAV-type modes have demonstrated success in animal models of obesity, AHRF, and abdominal hypertension.
7️⃣ Recruitment maneuvers are not the same as time-dependent recruitment
Traditional RMs use pressure blasts over seconds. But these alveoli need minutes, not seconds, to open. Time-dependent recruitment is slower, more physiologic, and more sustainable.
8️⃣ Mass loading worsens heterogeneity — the core driver of VILI
A central theme of the article: Pressure isn’t the problem — pressure distribution is.
Mass-loaded lungs show wide variability in:
- regional opening pressures
- time constants
- collapse thresholds
This creates stress risers, accelerating VILI unless time is adjusted to stabilize units.
9️⃣ The horse and pig models validated the concept
In both the equine mass-loading model and porcine AHRF + ACS model, the authors showed:
- improved oxygenation
- improved compliance
- restored FRC
- reduced edema
- reduced tissue injury using a time-based ventilation strategy.
These findings support translating this approach to human AHRF and obesity.
🔟 This paper proposes a shift in how we think about ARDS ventilation
Rather than focusing exclusively on:
- Vt
- PEEP
- plateau
- driving pressure
We must consider:
- opening time
- collapse time
- time under pressure
- expiratory duration as a therapeutic variable
This represents a major conceptual evolution in lung-protective ventilation.
4. How This Should Influence Your Practice
- Stop relying on PEEP alone to fix mass-loading physiology — it won’t.
- Start thinking of time as a modifiable ventilation parameter.
- Shorten expiratory time to preserve alveolar stability.
- Consider long inspiratory times to support gradual recruitment.
- Recognize that the sickest, heaviest, or most mass-loaded patients often need physiologic strategies outside conventional ventilation.
5. What This Paper Does Not Prove
- It is not a clinical RCT; it’s a physiology-driven perspective supported by animal data.
- It does not establish a single “best mode,” but rather explains the mechanism behind time-dependent recruitment.
- It does not claim PEEP is useless — only that PEEP alone is insufficient in mass loading.
This is foundational physiology, not dogma.
6. Bottom Line for Clinicians
Mass-loaded lungs don’t fail because they lack pressure — they fail because they lack time.
In obesity, ACS, and AHRF, alveoli collapse faster and open slower than your ventilator is set to handle. The future of lung-protective ventilation will incorporate time, not just pressure, as a central therapeutic tool.
7. A Question for Our Readers
Do you routinely adjust inspiratory/expiratory time to counter mass loading — or is PEEP still your primary tool in obese and ACS patients?
As always, don’t forget to like, share, and subscribe. See you on the other side!
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

