1. Why this editorial matters — and why you should read it
ECMO teams across the world ask the same question daily:
“What hemoglobin level actually improves oxygen delivery in ECMO — and when does transfusion do more harm than good?”
Despite decades of ECMO evolution, there is still no evidence-based transfusion threshold for ECMO patients. This editorial exposes just how fragile our assumptions are — and challenges us to rethink a practice that consumes massive blood resources without clear patient benefit.
If you manage ECMO, this piece forces you to reconsider whether we transfuse based on habit, not physiology.
2. The article in 5 lines
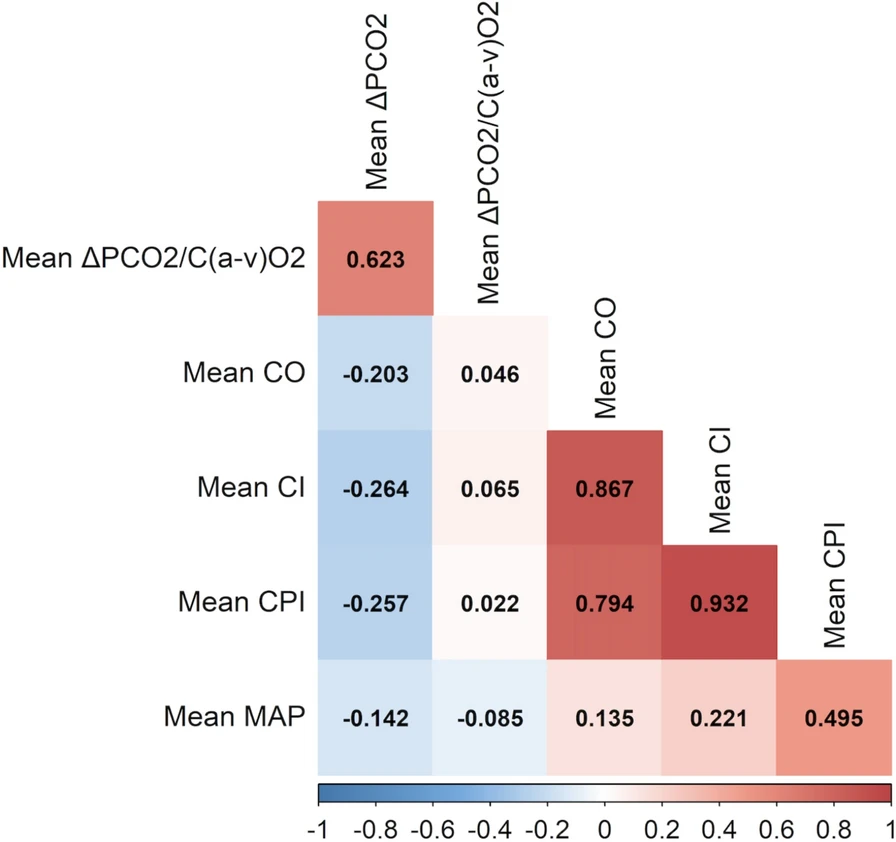
- ECMO can support global oxygen delivery (DO₂), but tissue oxygenation depends on microcirculation, RBC deformability, and oxygen extraction.
- Hemoglobin is the only modifiable component of DO₂ once ECMO flow is maxed out — but transfusion increases viscosity and may not improve microvascular flow.
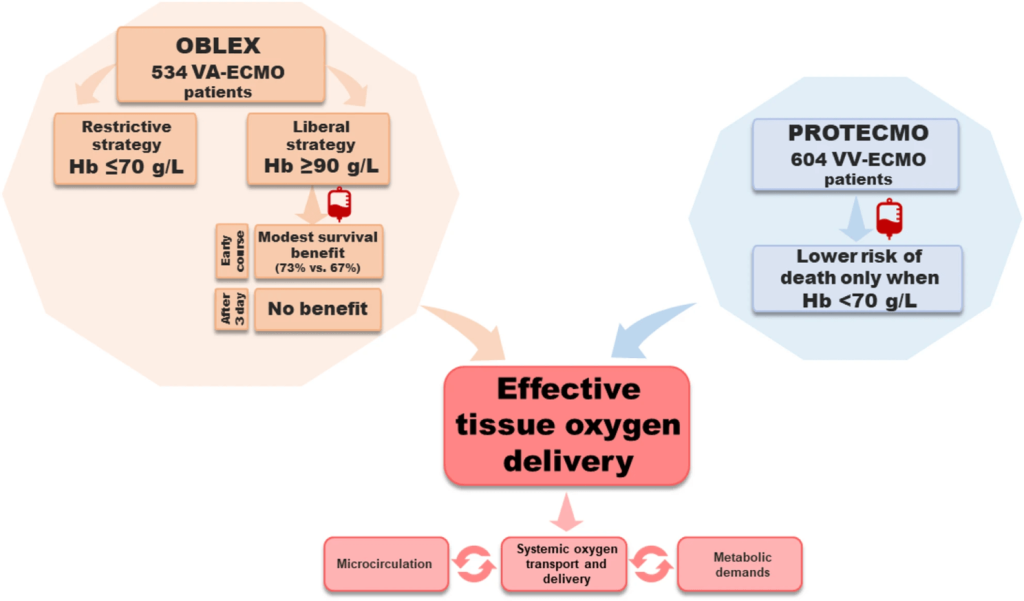
- Evidence for transfusion thresholds in VA-ECMO is weak: early observational data (OBLEX) suggested benefit from higher Hb, but this disappeared over time and is likely confounded.
- In VV-ECMO, the strongest data (PROTECMO) show benefit only when Hb < 7 g/dL, with no mortality improvement at higher levels.
- Experts and international societies agree: we do not know the right threshold, and ongoing trials aim to clarify this major gap in ECMO practice.
3. What they actually found — the clinically meaningful insights
1. ECMO patients are not normal anemic patients
Oxygen delivery depends on more than Hb: viscosity, RBC deformability, aggregation, and microvascular flow all determine whether transfusion truly increases DO₂. In critically ill inflammation, RBC deformability drops and viscosity rises — meaning transfusion may worsen microcirculatory flow, even if CaO₂ rises.
2. Hemoglobin alone is a poor transfusion trigger
Fluid shifts, hemodilution, and rapid changes in plasma volume make Hb an unreliable surrogate for oxygen delivery in ECMO patients. The central question becomes:
Are we treating a number or a physiologic need?
3. VA-ECMO physiology complicates everything
VA-ECMO creates two competing circulations that mix unpredictably in the aorta. Thus, oxygen delivery differs proximally and distally, making it unclear whether higher Hb is beneficial universally.
The OBLEX cohort (n = 534) suggested early survival benefit with liberal transfusion (Hb ≥ 9 g/dL), but this effect vanished later — and early bleeding likely confounded who ended up in the restrictive arm.
Bottom line: no convincing evidence that higher Hb improves outcomes in VA-ECMO.
4. VV-ECMO evidence is clearer: benefit only below 7 g/dL
The PROTECMO study (604 patients across 41 ECMO centers) found that transfusion improved survival only when Hb < 7 g/dL — and had no benefit above that threshold. This mirrors classic oxygen supply–dependency findings from older animal and human studies.
Thus, in VV-ECMO, restrictive transfusion appears safe — and potentially preferable.
5. Transfusion does more than raise hemoglobin — often in the wrong direction
Stored RBCs impair nitric oxide (NO) signaling, increase microvascular resistance, and can restrict blood flow to oxygen-dependent tissue beds. In ECMO, hemolysis and cell-free hemoglobin further scavenge NO, worsening vasodilation and potentially reducing tissue oxygenation despite higher CaO₂.
This explains why transfusion may fail to improve oxygen consumption (VO₂) in critically ill patients.
6. The rise of awake ECMO increases oxygen demand
Awake ECMO reduces sedation and promotes early mobilization — but this raises VO₂, making oxygen delivery even more dependent on microvascular function rather than simply Hb concentration.
This shift pushes us further toward individualized DO₂ assessment, not threshold-driven transfusion.
7. No society provides a clear ECMO transfusion threshold
- ELSO: no evidence that general ICU transfusion thresholds apply; ECMO patients are different.
- ESICM: recommends restrictive strategies for postoperative cardiac patients, but cannot provide ECMO-specific guidance.
We are officially operating in a gray zone, guided more by habit than data.
8. Trials are underway to finally answer this question
Several ongoing RCTs — TREC, ROSETTA, TITRE, ICONE — aim to determine whether restrictive or liberal strategies truly improve outcomes. Until then, clinicians must use physiology, not arbitrary numbers.
4. How this editorial should change your practice
1. Question every transfusion
Because ECMO patients often have microcirculatory and rheologic impairments, transfusion does not guarantee improved DO₂ — and may worsen microvascular oxygen delivery.
2. Transfuse for physiology, not for hemoglobin
Look for:
- Rising lactate
- Signs of supply-dependency
- Low venous saturation in mixed venous blood
- Clinical evidence of poor perfusion
- Hemodynamic changes during sweep or ECMO flow adjustments
3. ESG: “ECMO Should Guide”
Let the patient’s metabolic demands and circulatory physiology guide your decision — not a static Hb target.
5. Bottom line for clinicians
ECMO does not break physiology — it magnifies it. The belief that “higher hemoglobin = better oxygen delivery” is not supported by current evidence in ECMO.
The best available data suggest:
- VV-ECMO: benefit from transfusion only when Hb < 7 g/dL.
- VA-ECMO: unclear benefit; evidence does not support liberal thresholds.
Until ongoing trials give us clarity, the safest and most physiologically grounded approach is:
Transfuse the right patient, at the right moment, for the right physiologic reason — not because Hb crossed an arbitrary line.
6. A question for our readers
How low is “too low” for hemoglobin in your ECMO practice — and do you use physiology (VO₂/DO₂ markers, lactate, SvO₂) to guide transfusion decisions rather than a fixed number?
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.