Abstract
This perspective challenges one of the most fundamental assumptions in ARDS ventilation: that only inspiratory forces (tidal volume, driving pressure, plateau pressure, mechanical power) shape lung injury. The authors argue that expiratory time—specifically, the rate of lung emptying—is an overlooked determinant of stress and strain.
In injured lungs with low compliance and heterogeneous time constants, rapid expiration may generate harmful regional pressure gradients, promoting “implosive” injury as unstable units collapse too quickly. Conversely, excessively prolonged expiration risks de-recruitment and cyclic collapse.
The authors propose that controlling expiratory duration may become a missing pillar of lung-protective ventilation, complementing tidal volume reduction, plateau pressure limitation, and optimized PEEP. They highlight the need for individualized management based on lung mechanics, time constants, and the balance between maintaining alveolar stability and preventing overdistension.
Key Insights
1️⃣ Lung injury does not occur only on inspiration — expiration matters too
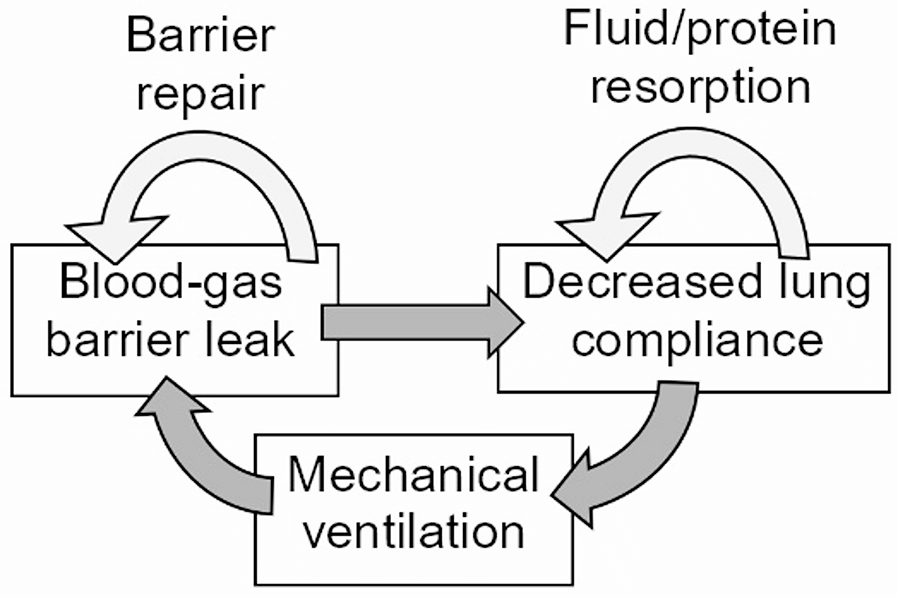
Traditionally, VILI has been attributed to inspiratory overdistension and cyclic stretching. The authors emphasize that expiration can also impose injury through rapid pressure shifts and dynamic compression of unstable alveoli, especially in heterogenous ARDS lungs with mismatched time constants.
2️⃣ Injured lungs empty unevenly due to time-constant heterogeneity
Regions with short time constants empty quickly, while those with long time constants empty slowly. Rapid global expiration may cause “implosive” collapse of vulnerable units, producing shear stresses comparable to the damaging forces seen during injurious inflation.
3️⃣ Classical lung-protection strategies focus only on inspiration
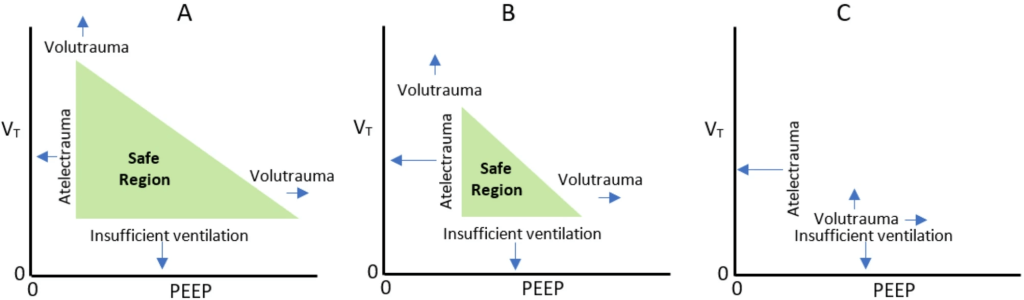
Low tidal volume, low plateau pressure, optimized PEEP, and driving pressure reduction form the modern protective framework. However, these fail to address how the lung deflates, which may expose certain regions to abrupt collapse, deformation, and shear.
4️⃣ Expiratory flow limitation becomes clinically important
In injured lungs, expiratory flow may become too fast relative to regional mechanical properties. This creates transient but significant pressure gradients between units, a phenomenon that can amplify mechanical stress and propagate injury.
5️⃣ Too short an expiratory time may produce “implosive atelectrauma”
The article describes how rapid deflation can cause immediate collapse of unstable alveoli, generating shear forces that resemble dynastic collapse injury. This mechanism may operate in parallel with classical atelectrauma during inspiration and warrants targeted mitigation.
6️⃣ Too long an expiratory time risks derecruitment
Prolonging expiratory duration to prevent rapid collapse may inadvertently promote cyclic derecruitment, particularly when PEEP is insufficient to maintain end-expiratory lung volume. Thus, expiratory timing—like PEEP—must be titrated individually.
7️⃣ The ideal expiratory duration is personalized, not fixed
The authors state that expiratory time must be tailored to the patient’s:
- compliance
- resistance
- regional time constants
- lung heterogeneity
- stability of dependent regions
This parallels the shift from fixed tidal volumes to individualized driving pressure targets.
8️⃣ Flow-controlled expiration (FCE) may reduce expiratory injury
Constraining expiratory flow—via decelerated or flow-controlled expiration—can reduce shear and maintain alveolar interdependence. Early data suggest FCE may improve gas exchange and reduce mechanical heterogeneity, though clinical trials are needed.
9️⃣ The authors call for expiratory parameters to be integrated into VILI frameworks
The modern VILI model integrates energy, power, strain, stress, and frequency of cycling. The article argues that expiratory flow velocity and expiratory timing should be added to this framework as quantifiable, modifiable contributors to injury.
🔟 Future research must investigate expiratory-time–driven injury mechanisms
The authors highlight urgent research needs in:
- quantifying “implosive injury”
- integrating expiratory timing into ventilator algorithms
- identifying optimal expiratory flow patterns
- testing FCE in clinical ARDS
- building bedside tools to measure expiratory strain
This may redefine lung-protection as a both-phases intervention, not inspiration-only.
Clinical Takeaways
- Expiration is not passive—it can harm the lung when too rapid or too prolonged.
- Time-constant heterogeneity in ARDS predisposes patients to expiratory shear injury.
- Clinicians should begin considering expiratory flow and timing as modifiable variables.
- Future ventilators may include tools to modulate expiratory flow (e.g., FCE).
- Protective ventilation may evolve to include both-phase strategies, not inspiration-focused alone.
Conclusion
This perspective challenges decades of assumptions by asserting that the injured lung is vulnerable not only during inspiration but also during expiration—particularly when expiratory flow is rapid relative to regional mechanical time constants. As the field moves toward more personalized ventilation strategies, expiratory timing may become a crucial and currently overlooked parameter. Incorporating expiratory mechanics into lung-protective ventilation could fundamentally reshape how we ventilate ARDS patients in the coming years.
Discussion Question
Should expiratory flow and expiratory duration be formally incorporated into lung-protective ventilation protocols—similar to tidal volume, PEEP, and driving pressure?
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.Bates, J.H., Kollisch-Singule, M., Gaver, D.P. et al. Toward optimal mechanical ventilation of the injured lung: the role of expiratory duration. Crit Care 29, 481 (2025). https://doi.org/10.1186/s13054-025-05683-2

