In the last newsletter, we discussed the roles of driving pressure (DP) [DOI: 10.1056/NEJMsa1410639] and mechanical power (MP) [DOI 10.1007/s00134-016-4505-2] as factors contributing to ventilator-induced lung injury (VILI) in patients with acute respiratory distress syndrome (ARDS). Neither DP nor MP directly causes lung damage; instead, they serve as markers indicating that VILI (excessive strain) is likely occurring. The correlation of MP with outcomes improves significantly when normalized to respiratory system compliance (CRS) or end-expiratory lung volume (EELV). [doi.org/10.1186/s13054-020-02963-x]
The question now is, as a clinician managing the ventilator for a patient developing ARDS, how should I respond to the increasing DP and MP as the lung progressively collapses and CRS falls? Dr. John Marini is a friend, colleague, and a leader in the field of protective lung ventilation. His editorial, “How I optimize power to avoid VILI,” describes Dr. Marini’s approach. [doi.org/10.1186/s13054-019-2638-8]
Tidal volume (VT) is adjusted to maintain DP 15 cmH2O and a plateau pressure of 27 cmH2O. Inspiratory flow is modulated to keep an I:E ratio between 1:1.5 and 1:1. Because excessive MP has been shown to correlate with outcomes (especially when normalized to CRS and EELV), Dr. Marini attempts to downregulate each of the power’s determinants, as indicated. [doi.org/10.1186/s13054-019-2638-8]
This is a great approach if you decide to constrainyourself to ventilating a heterogeneously ventilated lung with low EELV and CRS. After all, what else can you do but lower the DP and MP by adjusting the ventilator settings?
What if you could normalize EELV and CRS? Then, DP and MP would be lower for any given set of ventilator settings. Indeed, it has been shown that if MP is not normalized to EELV and CRS, then it does not correlate with outcomes. [doi.org/10.1186/s13054-020-02963-x]
Our group has demonstrated that, in conjunction with other ventilator settings, inspiratory and expiratory times can be used to stabilize the lung and then gradually reopen it (hours or days). [doi.org/10.3390/jcm12144633] By normalizing EELV and CRS, it dramatically reduces excessive lung strain regardless of DP and MP. Figure 1 shows an ARDS patient on conventional ventilation (A. Day 0) and then converted to time-controlled ventilation (B-D, Days 1-3). [doi.org/10.1186/s13054-022-04105-x] Using conventional ventilation (A) with relatively short inspiratory and long expiratory times, the lung is collapsed (X-ray) with a low EELV, and CRS is low (18 ml/cmH2O). VT is set low (6.2 ml/kg), but DP remains high (24 cmH2O) due to the low CRS.
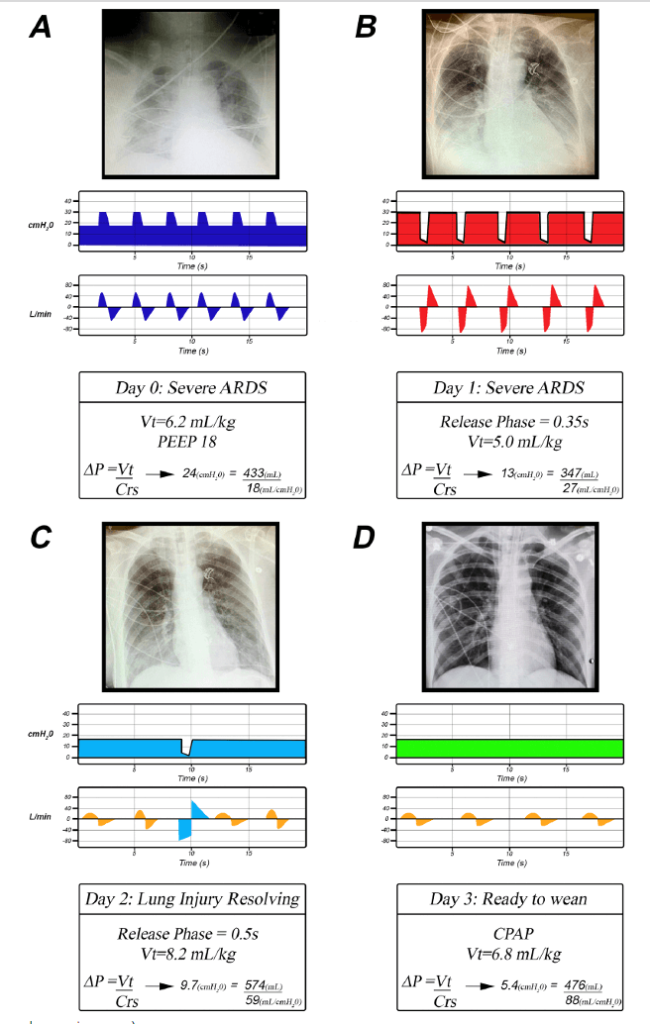
B) Switching to time-controlled ventilation on Day 1. The extended inspiratory time recruits a small volume with each breath, and the very brief expiratory time prevents the newly opened tissue from re-collapsing. The lung has opened (X-ray), increasing EELV and CRS (27 ml/cmH2O). The Release Phase during exhalation is very short (0.35 seconds), preventing tissue re-collapse and maintaining a low VT (5.0 ml/kg). Combined low VT and higher CRS reduce DP (13 cmH2O). C,D) Show the progressive lung recruitment (X-ray) and increasing CRS over the next two days that drop the DP into the normal range (9.7 and 5.4 ml/cmH2O). The gold flow/time waveforms are spontaneous breaths, and the number of Release Phases can be reduced as the patient generates adequate minute ventilation (VE). [doi.org/10.1186/s13054-022-04105-x]
Time-controlled ventilation is not constricted to ventilating a lung with low EELV and CRS, but rather ratchets the lung open one breath at a time. [doi: 10.3389/fphys.2023.1287416] This can occur in less than 24 hours, as shown in the example (Fig. 1B). As can be seen, DP is significantly reduced after the lung is reopened due to the elevation of CRS even with a higher VT (A. VT 6.2 ml/kg with DP = 24 cmH2O; C. VT 8.2 ml/kg with DP = 9.7 cmH2O). [doi.org/10.1186/s13054-022-04105-x]
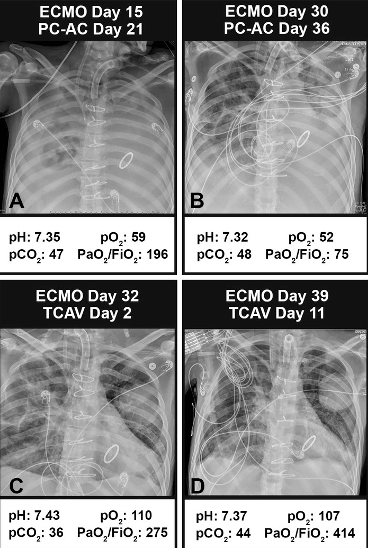
A case study highlights the difference between a ventilation strategy that keeps the lung collapsed and one that ratchets it open. A patient who had severe ARDS was on pressure-control assist-control (PC-AC) mode using the ARDSnet low VT ventilation protocol for 36 days and on extra-corporal membrane oxygenation (ECMO) for 36 days (Fig. 2 A, B). The lung remained collapsed (X-ray), and blood gases were poor. Switching to the time-controlled adaptive ventilation (TCAV) method to set and adjust the airway pressure release ventilation (APRV) mode, the lung gradually reopened over 2 days, and by day 11, the patient was decannulated, extubated, and ultimately discharged home (Fig. 2C, D). [doi.org/10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts.A5189]
In conclusion, rising driving pressure and mechanical power are not the cause of injury—they are warnings that ventilation is being delivered into a small, collapsed, low-compliance lung. Simply lowering ventilator settings treats the symptoms, not the problem. By restoring EELV and improving compliance through time-controlled ventilation, the lung can be stabilized and reopened, reducing strain regardless of the absolute tidal volume or mechanical power.
In the end, it is not how much energy we deliver, but the condition of the lung receiving it. A collapsed lung cannot be safely ventilated. A reopened lung can.

