Summary
Why This Study Matters
This study provides rare human clinical data linking spontaneous breathing during AHRF, ventilation distribution on EIT, and systemic inflammation (IL-6). It helps clarify when transitioning from non-invasive support to controlled mechanical ventilation may reduce physiologic stress and potential P-SILI.
1. What the Investigators Wanted to Know
The study examined whether AHRF patients who transition early to controlled mechanical ventilation (CMV) demonstrate lower inflammation and more homogeneous ventilation compared with those kept on spontaneous breathing (SB).
- Focus on IL-6 and IL-8 changes over 24 hours
- Measurements using electrical impedance tomography (EIT)
- Comparison of oxygenation, physiology, and ventilation distribution
This addresses a central question in modern ARDS management: Does prolonged high-drive spontaneous breathing worsen inflammation?
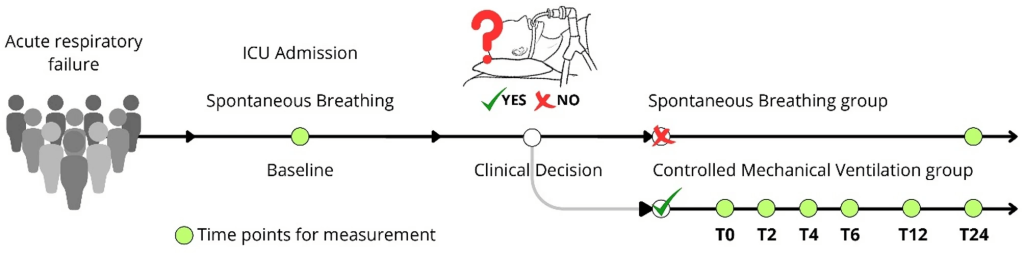
2. Study Design and Population
This was a prospective observational cohort from a single ICU in Chile between 2018–2021.
- 40 adults with acute hypoxemic respiratory failure (PaO₂/FiO₂ ≤ 300 on FiO₂ ≥ 0.30)
- No COPD exacerbation, no cardiogenic pulmonary edema, no hypercapnia, no immediate need for intubation
- Most patients began on high-flow nasal cannula
Two clinician-determined groups emerged:
- Spontaneous Breathing (SB): 12 patients remained on non-invasive support for 24 hours
- Controlled Mechanical Ventilation (CMV): 28 patients were intubated and placed on lung-protective ventilation within 24 hours
This design reflects real-world decision-making, not a randomized protocol.
3. Physiologic Changes After Moving to Controlled Mechanical Ventilation
Patients who transitioned to CMV showed substantial physiologic “unloading.”
- Respiratory rate decreased (32 → 24/min)
- Heart rate decreased (102 → 86 bpm)
- Temperature decreased slightly
- PaCO₂ rose slightly as hyperventilation resolved
- pH fell modestly but remained acceptable
These patterns reflect reduced work of breathing and stabilization under lung-protective ventilation.
Oxygenation also improved significantly.
- PaO₂/FiO₂ increased from ~140 at baseline to ~199 at 24 hours
This indicates better alveolar recruitment and improved respiratory mechanics.
4. Ventilation Distribution and Recruitment on EIT
EIT demonstrated meaningful improvements in the CMV group.
- Global Inhomogeneity Index (GI) decreased (more homogeneous ventilation)
- End-expiratory lung impedance (EELI) increased (larger end-expiratory lung volume)
- Impedance ratio shifted toward dependent regions (more balanced ventilation)
These changes align with established mechanisms of controlled ventilation: recruitment, stabilization, and reduction of pendelluft and regional overdistension.
This contrasts sharply with the SB group, where EIT patterns remained unchanged.
5. Systemic Inflammation: The IL-6 Signal
The strongest signal in the study was the reduction of IL-6 in patients transitioned to CMV.
- IL-6 dropped from ~305 pg/mL at baseline to ~27 pg/mL at 24 hours
- IL-8 showed no significant change
The SB group showed no improvement in IL-6 or IL-8 across the same timeframe.
Although observational, the alignment of IL-6 decreases with improvements in ventilation homogeneity supports the idea that reducing effort and stabilizing the lung modulates inflammatory stress.
6. What Happened to Patients Left on Spontaneous Breathing
The SB group (n=12) demonstrated minimal physiologic or biological improvement.
- Respiratory rate decreased modestly
- Oxygenation showed no significant improvement
- EIT indices (GI, EELI, TVI) showed no meaningful changes
- IL-6 and IL-8 did not improve
At 24 hours, SB patients had:
- Lower PaO₂/FiO₂
- More heterogeneous ventilation on EIT
This suggests persistent respiratory effort, ongoing regional strain, and continued inflammatory stress.
7. Exploratory Predictors and Mechanistic Insights
The investigators performed exploratory analyses to identify predictors of intubation.
- Higher baseline respiratory rate
- Higher heart rate
- Lower PaO₂/FiO₂
All were associated with a higher likelihood of requiring CMV.
Additionally, improved impedance ratio over time was associated with lower IL-6 levels, reinforcing the concept that more homogeneous ventilation correlates with reduced systemic inflammatory load.
8. Clinical Interpretation for the Bedside
Although limited by its observational design, the findings support three important clinical principles.
1. High-effort spontaneous breathing in AHRF is not benign.
- No improvement in heterogeneity
- No improvement in gas exchange
- No reduction in IL-6
2. Controlled mechanical ventilation may rapidly stabilize physiology in selected patients.
- Lower HR and RR
- Improved oxygenation
- More homogeneous ventilation
- Significant reduction in IL-6
3. This study aligns with the P-SILI framework.
- High respiratory drive + heterogeneous lung regions → large pleural swings
- Pendelluft and strain may amplify inflammatory load
- Stabilizing the lung and reducing inspiratory effort may interrupt this cycle
This supports a lower threshold for intubation in patients with de novo AHRF who remain tachypneic, tachycardic, and hypoxemic despite optimized non-invasive support.
9. Important Limitations to Keep in Mind
- Observational design with confounding by indication
- Small cohorts, particularly the SB group
- Short follow-up (24 hours)
- Concurrent clinical interventions may influence inflammation
- Single center, limiting generalizability
These findings should generate hypotheses, not change guidelines—yet they offer valuable insight into bedside physiology.
10. Key Takeaways for Your Next ICU Shift
1. Persistent high-drive spontaneous breathing in AHRF may maintain heterogeneity and inflammation.
- SB patients showed no improvement in IL-6 or EIT parameters.
2. Controlled mechanical ventilation was associated with a sharp reduction in IL-6 and improved homogeneous ventilation.
- Suggests physiologic and biomechanical benefit when used early in sicker patients.
3. Simple bedside markers remain highly predictive of the need for intubation.
- Respiratory rate
- Heart rate
- PaO₂/FiO₂
These remain essential “red flags” during non-invasive trials.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.

