Abstract:
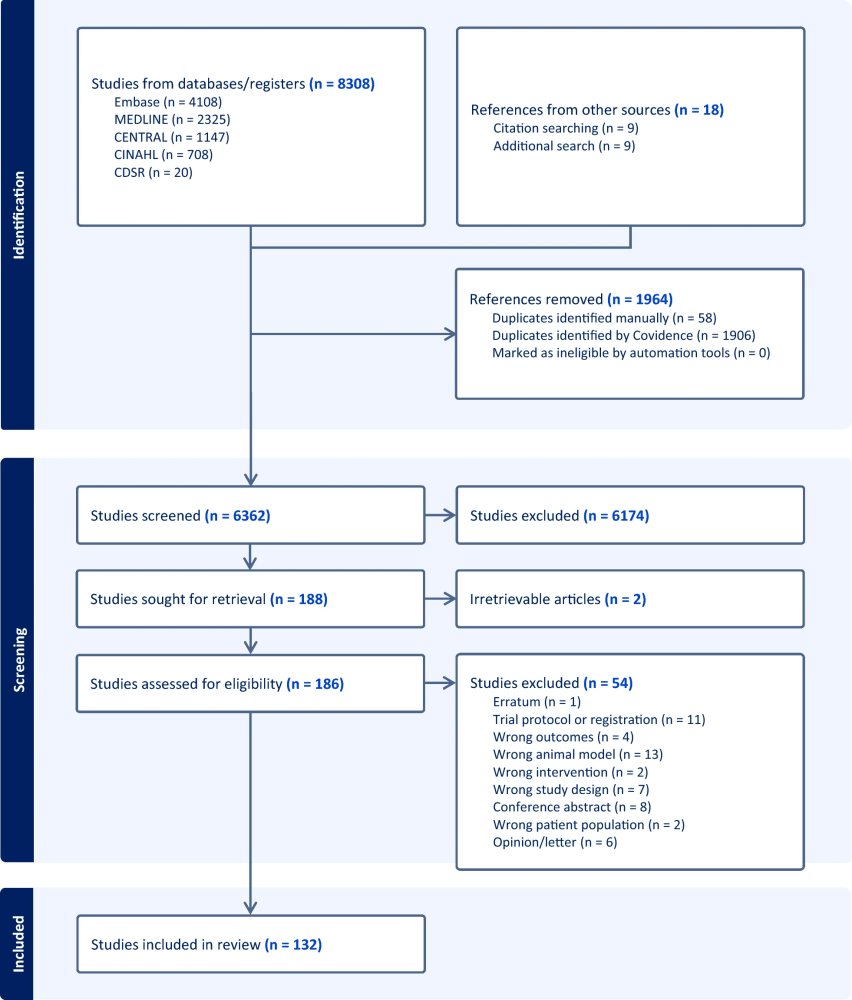
This scoping review maps all non-mechanical haemodynamic support used in acute pulmonary embolism (PE) while definitive clot-reducing therapy is pursued. Across animal studies, case series, observational cohorts, trials, and reviews, the authors catalogue vasopressors, inotropes, fluids, and pulmonary vasodilators. Evidence is heterogeneous and mostly low-quality; some agents improve physiological surrogates (CO, PVR, RV function), but robust outcome data are sparse, and standardized recommendations are limited.
Key Insights:
- Scope of evidence: 57 agents identified across animal and human studies; human data are dominated by small, non-randomized reports.
- Vasopressors: Agents like norepinephrine are frequently used to restore systemic pressure and RV coronary perfusion; comparative human data remain limited.
- Inotropes: Dobutamine and phosphodiesterase-3 inhibitors (e.g., milrinone) can augment RV contractility but may precipitate hypotension without concurrent vasopressor support.
- Pulmonary vasodilators: Inhaled nitric oxide and prostacyclin analogues (e.g., epoprostenol/iloprost) reduce RV afterload and improve short-term haemodynamics; clear survival benefit is unproven.
- Fluids: Excess preload can worsen RV dilation and septal shift; the mapped literature supports cautious, small-volume fluid strategies rather than aggressive boluses in shock unless hypovolaemia is evident.
Why This Matters:
Right-ventricular failure drives early mortality in acute PE. This review clarifies what we think helps (pressors, selective inotropes, inhaled vasodilators, cautious fluids) versus what we know—highlighting the evidence gaps that should shape protocols and trials.
Conclusion:
Non-mechanical haemodynamic support in acute PE is biologically plausible and physiologically helpful in small studies, but high-quality outcome evidence is lacking. Practice should prioritize norepinephrine-anchored MAP support, selective inotropy when low output is present, inhaled vasodilators for RV afterload, and judicious fluids, while the field pursues prospective, adequately powered trials.
Take-Home for Clinicians:
- Stabilize MAP (often with norepinephrine) to protect RV perfusion; add inotrope only when output is low, and pair with a pressor if needed.
- Use inhaled pulmonary vasodilators to unload the RV when available; expect haemodynamic, not proven survival, gains.
- Avoid large fluid boluses in the absence of clear hypovolaemia; cautious preload is safer for the strained RV.
Discussion Question: If you could test one bedside bundle tomorrow (pressor-anchored MAP target + selective inotropy + inhaled vasodilator + restrictive fluids), which single objective trigger would you use to start/stop each element?
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.

