Legionella Pneumonia in the ICU: Does ECMO Improve Outcomes?
Abstract:
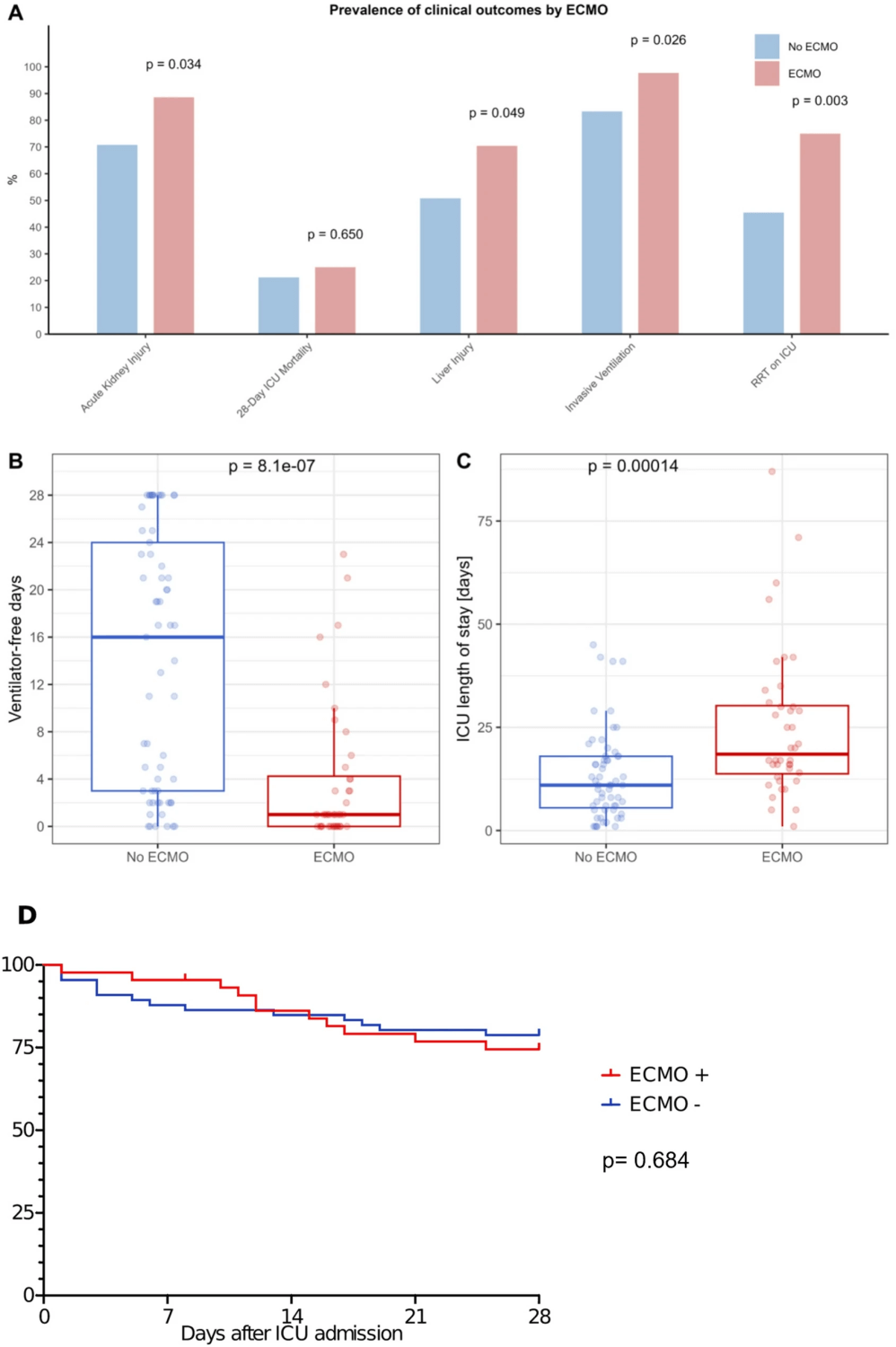
This multicenter, retrospective cohort study (Zurich, Hannover, Bonn; 2013–2023) evaluated 110 ICU patients with Legionella pneumonia (LP). Severe LP frequently progressed to ARDS and multiorgan failure; 40% required ECMO. Despite greater severity (SOFA 12 vs 9), ECMO patients had similar 28-day mortality (25% vs 21%) compared to non-ECMO. Importantly, LP-associated ARDS on ECMO showed lower mortality than typically reported in general ARDS cohorts.
Key Insights:
- Cohort profile: Median age 60; 75% male; 89% required invasive ventilation; 40% received ECMO (mostly VV).
- ECMO outcomes: Despite higher illness severity, ECMO patients achieved mortality rates comparable to non-ECMO, suggesting a potential survival benefit in LP-ARDS.
- Antibiotic adequacy: Only 57% had Legionella-specific coverage at ICU admission. Delayed therapy correlated with fewer ventilator-free days and longer ICU stays, though not higher mortality.
- Risk factors for death: Independent predictors were hospital-acquired LP (OR 28.4) and elevated lactate (OR 1.31 per mmol/L).
- AKI & sepsis burden: AKI occurred in 78% overall, 89% with ECMO; septic shock in 66% of ECMO patients.
Why This Matters: For ICU teams, these findings support ECMO as a rescue option in severe LP-ARDS. LP patients may represent a subgroup with better ECMO survival than broader ARDS populations.
Conclusion: LP with ARDS carries high morbidity, but ECMO may equalize survival despite greater severity. Prompt Legionella-directed antibiotics remain essential, while hospital-acquired LP signals poor prognosis.
Take-Home for :
- ECMO should be considered for LP-ARDS with refractory hypoxemia.
- Ensure early Legionella coverage (macrolide or fluoroquinolone) at ICU admission.
- Watch lactate closely; >3.6 mmol/L predicts higher mortality.

Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.

