Abstract
Not all patients with refractory hypoxemia meet ECMO criteria — yet many still face catastrophic oxygenation failure with limited options. This study describes a physiology-guided “Lung Rescue Team (LRT)” model, designed to evaluate patients who are ineligible or borderline for ECMO by integrating mechanical ventilation physiology, multimodal imaging, hemodynamics, gas exchange, and lung recruitability profiling.
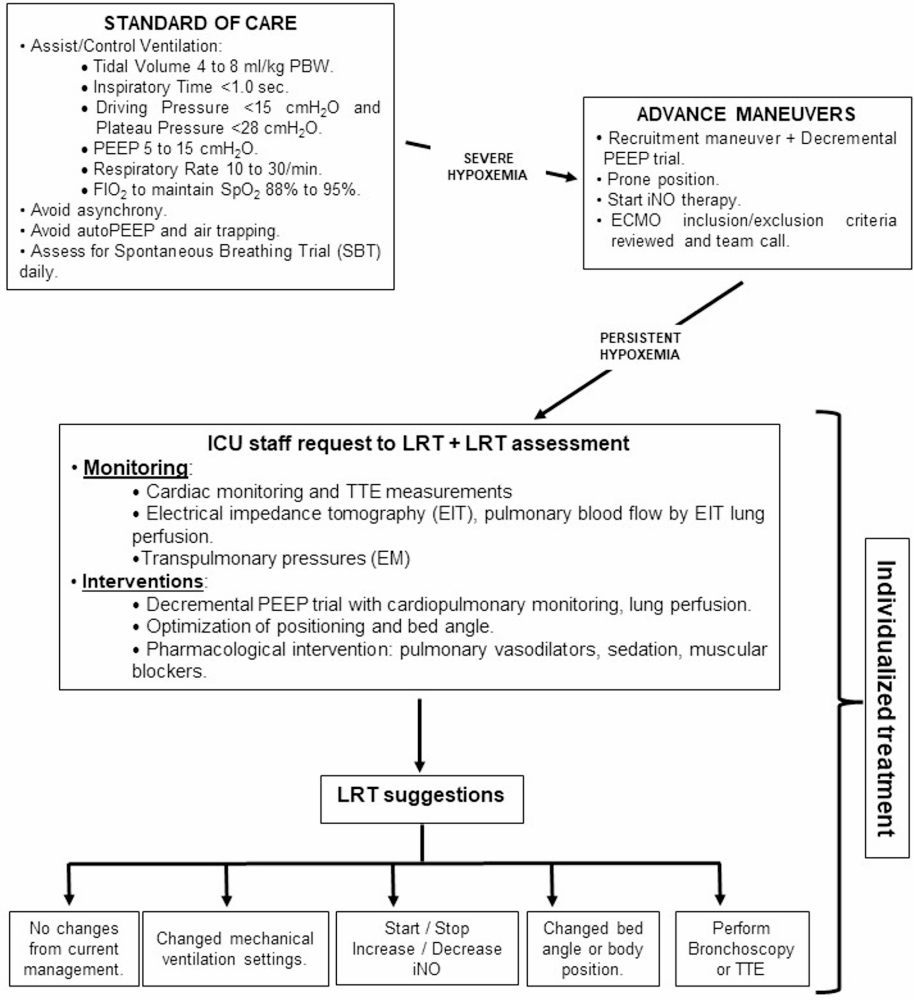
The LRT uses structured algorithms to characterize the mechanism of hypoxemia (shunt, low VA/Q, dead space, or low EELV), identify reversible physiology, and apply targeted rescue strategies including personalized PEEP titration, recruitment assessment, prone positioning, inhaled pulmonary vasodilators, right-ventricular optimization, and extracorporeal “alternatives.”
This approach provides a reproducible framework for managing patients who cannot access ECMO but remain at high risk of death, focusing on physiology restoration instead of escalating support blindly.
🔍 10 Key Insights
1️⃣ Not All Severe Hypoxemia Is the Same — Mechanisms Matter
The LRT approach begins with classifying hypoxemia based on mechanism, not severity alone. Using ABGs, lung mechanics, EIT, CT imaging, and bedside ultrasound, the team identifies whether the dominant driver is shunt, low VA/Q mismatch, derecruitment, dead space ventilation, or circulatory impairment.
2️⃣ A Dedicated Lung Rescue Team Bridges the Gap When ECMO Is Not an Option
Many patients were too old, too frail, too comorbid, or too late in their disease trajectory to qualify for ECMO. The LRT framework offers an organized multidisciplinary alternative, integrating intensivists, respiratory therapists, cardiologists, imaging specialists, and ECMO clinicians into one cohesive decision-making unit.
3️⃣ Recruitability Drives Ventilator Strategy — Not Fixed Protocols
LRT evaluation emphasizes recruitability testing, using tools such as:
- Pressure-volume loops
- CT aeration analysis
- EIT-derived distribution
- Response to incremental PEEP or prone positioning
Patients with high recruitability benefit from structured recruitment maneuvers and PEEP optimization, while low-recruitability lungs require gentler strategies to avoid overdistension.
4️⃣ Personalized PEEP Titration Prioritizes RV Protection
Instead of applying ARDSNet-style fixed tables, the LRT uses physiological endpoints such as:
- Driving pressure (ΔP)
- End-expiratory lung volume (EELV)
- RV performance
- Compliance response The goal is to balance oxygenation improvement without precipitating acute cor pulmonale.
5️⃣ Prone Positioning Is a Core Diagnostic and Therapeutic Tool
Proning is used not only to improve oxygenation, but to identify whether the lung’s physiology is recruitable, redistributable, or fixed. In some cases, the prone response helped redirect a patient toward alternative rescue therapies.
6️⃣ Pulmonary Vasodilators Are Targeted, Not Routine
Inhaled nitric oxide and inhaled prostacyclin are applied selectively, especially when RV dysfunction or vascular dysregulation is suspected. The LRT avoids reflexive vasodilator use without clear physiology-based justification.
7️⃣ Right-Ventricular (RV) Physiology Directly Guides Ventilation
Bedside echocardiography and hemodynamic assessment are key. The team differentiates between:
- Hypoxemia dominated by alveolar collapse, requiring PEEP
- Hypoxemia dominated by RV failure, requiring lower intrathoracic pressures, gentle ventilation, and vasoactive optimization
This prevents treatment strategies that inadvertently worsen the patient’s physiology.
8️⃣ EIT and Advanced Monitoring Are Integrated Into Real-Time Decisions
Electrical impedance tomography (EIT) provides continuous visualization of:
- Regional ventilation
- Pendelluft
- Derecruitment
- Overdistension
- Response to PEEP changes
This bedside imaging plays a central role in safely tailoring mechanical ventilation.
9️⃣ “Lung Rescue” Pathways Reduce Unnecessary ECMO Activation
Many patients initially thought to require ECMO improved once individualized physiological corrections were applied — avoiding futile ECMO referrals while improving outcomes for those who could be salvaged through targeted non-ECMO strategies.
🔟 A Structured Framework Creates Predictable, Reproducible Decision-Making
The LRT pathway allows clinicians to navigate severe hypoxemia with a methodical, physiology-anchored process, replacing chaotic trial-and-error approaches. This standardization ensures consistency across providers and enhances safety for high-risk patients.
Clinical Takeaways
- Severe hypoxemia should be approached with mechanism-based diagnostics, not protocol-driven ventilation alone.
- ECMO ineligibility does not mean therapeutic futility — physiology-guided interventions can reverse life-threatening hypoxemia.
- LRTs promote consistent, multidisciplinary, real-time decision-making.
- Tools like EIT, targeted PEEP titration, prone response, and hemodynamic integration are key to safe rescue.
- This model provides a template for institutions without ECMO programs to apply advanced physiology-based care safely.
Discussion
Can physiology-guided rescue strategies close the gap for hospitals without ECMO access — or will ECMO remain the ultimate failsafe for severe hypoxemia?
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.