Surgical Procurement of a Donor Heart with Complex Congenital and Venous Anomalies

Surgical Procurement of a Donor Heart with Complex Congenital and Venous Anomalies: PLSVC, Coronary Sinus Dilation, RA Aneurysm, and Patent Ductus Arteriosus (PDA)
In thoracic organ transplantation, discovering complex congenital and venous anomalies in a donor organ is a high-stakes scenario. While an isolated persistent left superior vena cava (PLSVC) is relatively common, its combination with massive coronary sinus (CS) dilation, a right atrial (RA) aneurysm, and a patent ductus arteriosus (PDA) presents unique surgical challenges.
Failure to plan for these anomalies during procurement can lead to:
Incomplete cardioplegic delivery (due to retrograde cardioplegia runoff into the PLSVC).
Severe right atrial wall fragility or tearing (from the RA aneurysm).
Massive pulmonary artery runoff and failure to arrest/protect the left ventricle (from an unligated PDA).
Unusable venous cuffs during the recipient implant.
With careful dissection and anatomical modifications, this complex organ can be safely procured and successfully transplanted.
Understanding the Interconnected Pathophysiology
To protect and explant this heart, the procurement surgeon must understand how these anomalies interact:
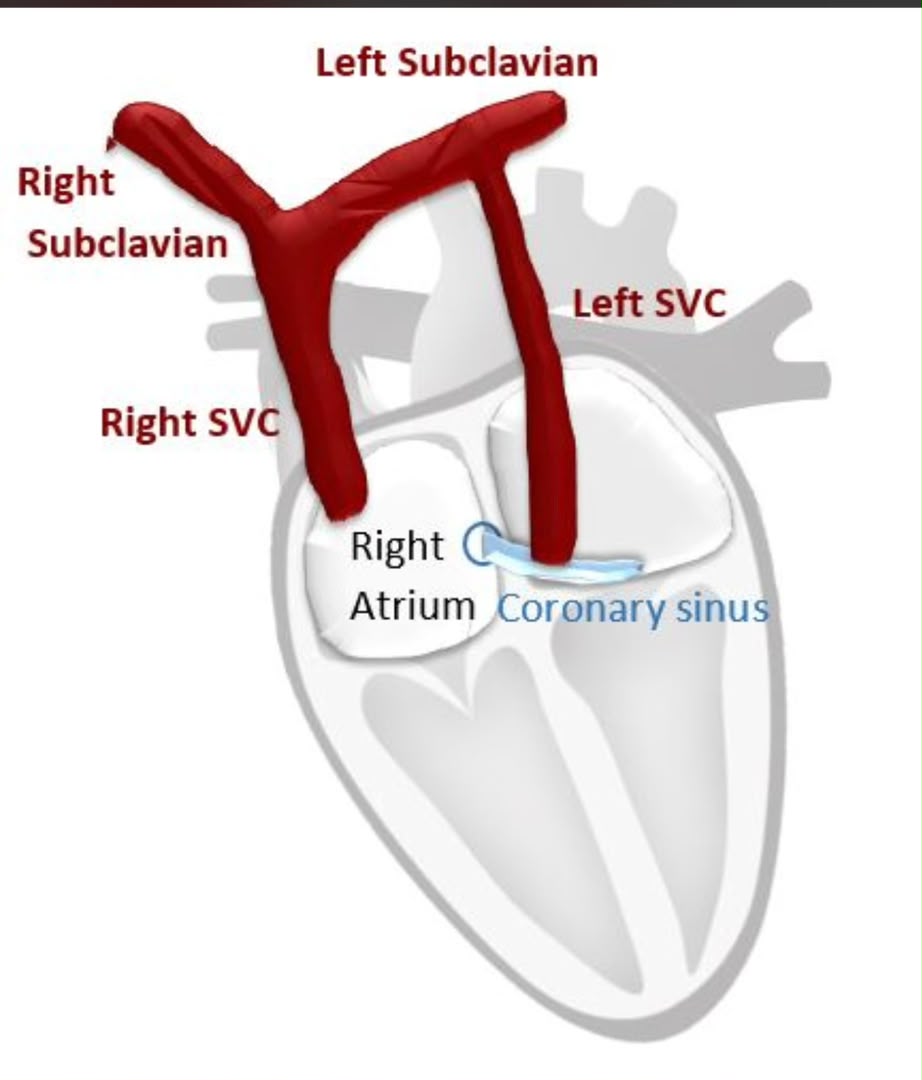
1. PLSVC and Dilated Coronary Sinus: The PLSVC results from a failure of the left anterior cardinal vein to regress during embryonic development. It travels down the left lateral mediastinum, anterior to the left hilum, and enters the left atrioventricular groove to drain into the coronary sinus. This continuous high-volume flow of systemic venous blood directly causes the dilation of the coronary sinus.
2. RA Aneurysm: The right atrial aneurysm may be a congenital diverticulum or a thin, paper-like wall segment resulting from chronic volume overload. This tissue is extremely fragile and must be handled with utmost care.
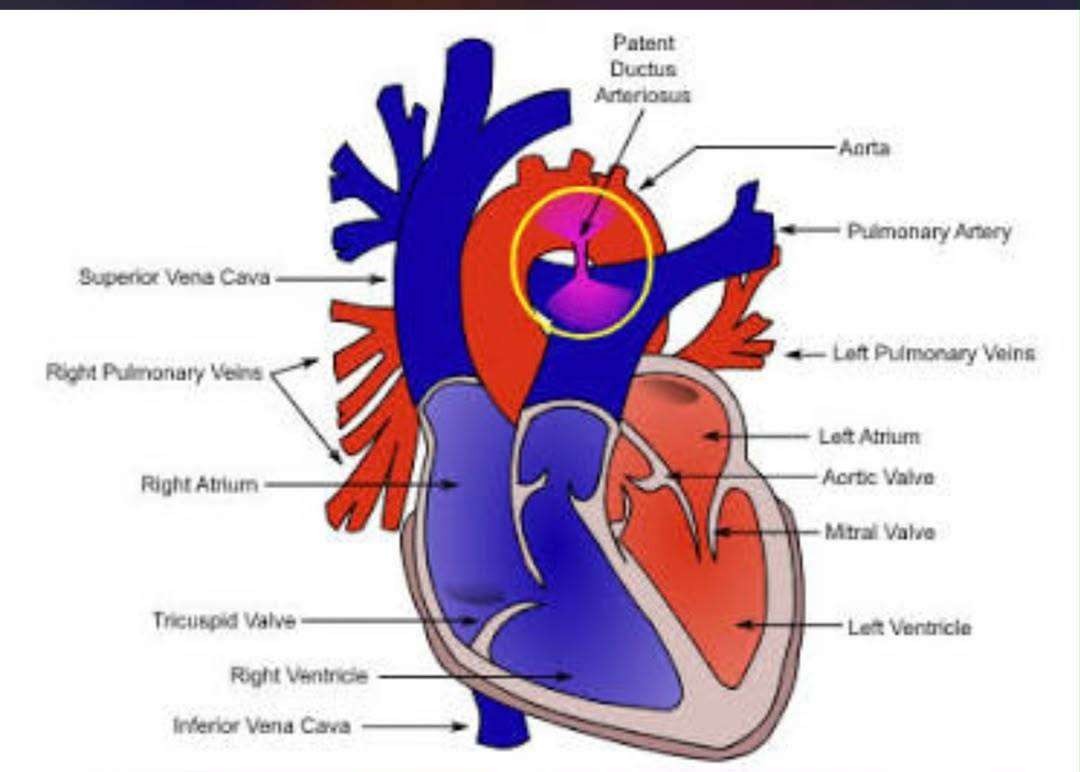
3. Patent Ductus Arteriosus (PDA): The PDA provides a direct connection between the main pulmonary artery (PA) and the descending aorta. During the administration of anterograde cardioplegia, if the PDA is not clamped or ligated, cardioplegia will shunt directly into the pulmonary vasculature. This causes left-sided volume overload, prevents adequate diastolic arrest, and risks ischemic injury.
In thoracic organ transplantation, discovering complex congenital and venous anomalies in a donor organ is a high-stakes scenario. While an isolated persistent left superior vena cava (PLSVC) is relatively common, its combination with massive coronary sinus (CS) dilation, a right atrial (RA) aneurysm, and a patent ductus arteriosus (PDA) presents unique surgical challenges.
Failure to plan for these anomalies during procurement can lead to:
Incomplete cardioplegic delivery (due to retrograde cardioplegia runoff into the PLSVC).
Severe right atrial wall fragility or tearing (from the RA aneurysm).
Massive pulmonary artery runoff and failure to arrest/protect the left ventricle (from an unligated PDA).
Unusable venous cuffs during the recipient implant.
With careful dissection and anatomical modifications, this complex organ can be safely procured and successfully transplanted.
Understanding the Interconnected Pathophysiology
To protect and explant this heart, the procurement surgeon must understand how these anomalies interact:
1. PLSVC and Dilated Coronary Sinus: The PLSVC results from a failure of the left anterior cardinal vein to regress during embryonic development. It travels down the left lateral mediastinum, anterior to the left hilum, and enters the left atrioventricular groove to drain into the coronary sinus. This continuous high-volume flow of systemic venous blood directly causes the dilation of the coronary sinus.
2. RA Aneurysm: The right atrial aneurysm may be a congenital diverticulum or a thin, paper-like wall segment resulting from chronic volume overload. This tissue is extremely fragile and must be handled with utmost care.
3. Patent Ductus Arteriosus (PDA): The PDA provides a direct connection between the main pulmonary artery (PA) and the descending aorta. During the administration of anterograde cardioplegia, if the PDA is not clamped or ligated, cardioplegia will shunt directly into the pulmonary vasculature. This causes left-sided volume overload, prevents adequate diastolic arrest, and risks ischemic injury.

Dr.Sam Zeraatian Nejad Davani,
Cardiovascular and Thoracic Surgeon
Transplant and Thoracic Organs Recovery Surgeon
Director of Georgia Atlanta Procure on Demand Thoracic Organs Transplant and Procurement Surgery
S.Zeraatiannejaddavani@procureodx.com