Total trans septal approach and DCD rapid recovery

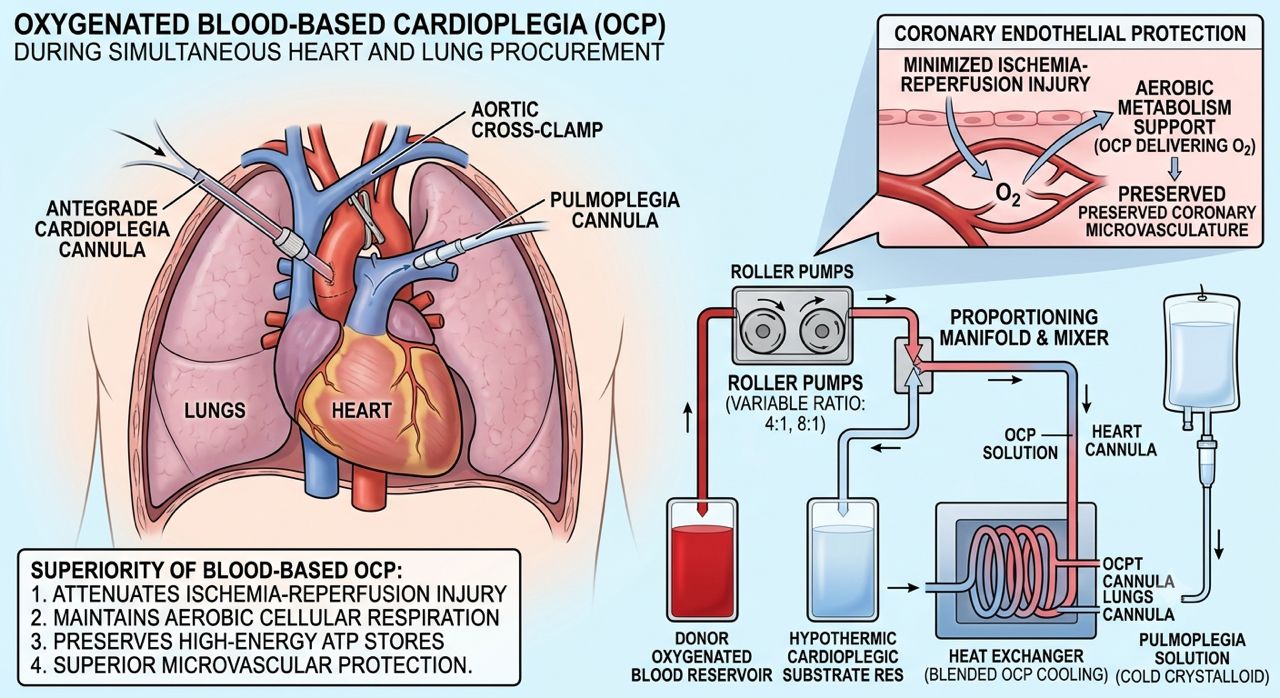
Oxygenated Cardioplegia (OCP) using a blood-based vehicle represents a significant shift from traditional cold crystalloid preservation during multi-organ heart and lung procurements. By leveraging a mixture of oxygenated donor blood and cold cardioplegic crystalloid substrate, this technique minimizes the profound metabolic shock of initial ischemia by maintaining aerobic cellular respiration and preserving high-energy intracellular phosphate stores (ATP). Its superiority lies in its ability to significantly attenuate ischemia-reperfusion injury (IRI), maintain coronary endothelial integrity, and offer superior microvascular protection—crucial factors when minimizing primary graft dysfunction in combined thoracic retrieval.
To execute this technique during procurement, once the donor is fully heparinized and the major thoracic structures are mobilized, an antegrade cardioplegia line is secured in the ascending aorta. A specialized delivery system or portable hypothermic perfusion circuit blends oxygenated donor blood with the hypothermic cardioplegic substrate (often in a 4:1 or 8:1 ratio). Following cross-clamp application and simultaneous venting of the right and left heart to prevent distension, the solution is delivered into the aortic root. Delivery pressures are tightly regulated—typically maintained below 150\text{ mmHg} to protect the coronary vasculature—while coordinating closely with the lung procurement team to ensure that concurrent anterograde pulmoplegia delivery and proper pulmonary venting prevent cross-contamination or systemic volume overload.
To execute this technique during procurement, once the donor is fully heparinized and the major thoracic structures are mobilized, an antegrade cardioplegia line is secured in the ascending aorta. A specialized delivery system or portable hypothermic perfusion circuit blends oxygenated donor blood with the hypothermic cardioplegic substrate (often in a 4:1 or 8:1 ratio). Following cross-clamp application and simultaneous venting of the right and left heart to prevent distension, the solution is delivered into the aortic root. Delivery pressures are tightly regulated—typically maintained below 150\text{ mmHg} to protect the coronary vasculature—while coordinating closely with the lung procurement team to ensure that concurrent anterograde pulmoplegia delivery and proper pulmonary venting prevent cross-contamination or systemic volume overload.



Dr.Sam Zeraatian Nejad Davani, Cardiovascular and Transplant surgeon. Advanced Fellow of Thoracic Organs Transplantation Chicago Illinois.