Partial Heart and Lung Transplantation with Two Recipients from One Donor

Partial Heart and Lung Transplantation: Maximizing Donor Organ Utilization Through Two-Recipient Transplantation
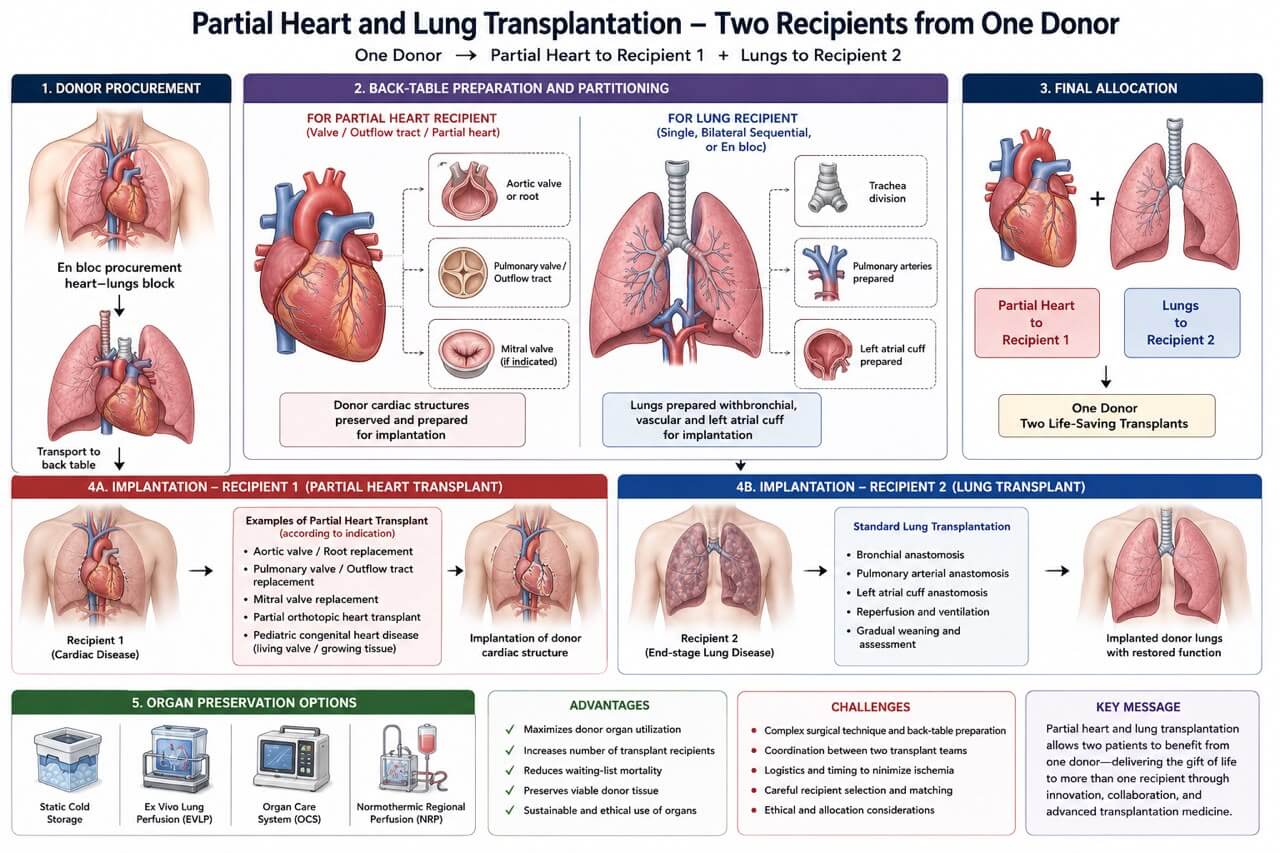
Partial heart and lung transplantation is an innovative organ utilization strategy that allows transplantation of thoracic organs from a single donor into two separate recipients. This approach aims to maximize the use of scarce donor organs while providing life-saving therapy to multiple patients from one donation.
Concept
Traditionally, the heart and lungs are transplanted either as individual organs or as a combined heart-lung block into a single recipient. In selected donors and recipients, however, only a portion of the donor heart is required for one recipient, while the lungs are transplanted separately into another recipient.
This strategy has become increasingly relevant with advances in organ preservation, ex vivo perfusion technologies, and complex reconstructive surgical techniques.
Donor Selection
Suitable donors should have:
* Excellent cardiac function with normal ventricular performance.
* Healthy lungs meeting standard lung transplantation criteria.
* No significant coronary artery disease or structural cardiac abnormalities.
* Stable hemodynamics with acceptable ischemic times.
* Favorable anatomical compatibility for both recipients.
Recipient Selection
Recipient 1 – Partial Heart Transplant
Candidates include patients requiring replacement of specific cardiac structures rather than the entire heart, such as:
* Aortic valve replacement using donor living valve tissue.
* Pulmonary valve replacement.
* Mitral valve reconstruction.
* Pediatric congenital heart disease requiring viable valve or outflow tract tissue.
* Patients undergoing partial orthotopic heart transplantation where native ventricular function can be preserved.
Recipient 2 – Lung Transplant
The second recipient undergoes:
* Single lung transplantation
* Bilateral sequential lung transplantation
* En bloc bilateral lung transplantation
depending on the underlying pulmonary disease.
Surgical Technique
Donor Operation
Following standard donor procurement:
1. Median sternotomy is performed.
2. Systemic heparinization is achieved.
3. Aortic cross-clamp is applied.
4. Cold cardioplegia is administered.
5. Pulmonary artery is flushed with preservation solution (e.g., Perfadex Plus).
6. The heart and lungs are removed en bloc.
The heart-lung block is transported to the back table.
Back-Table Preparation
The donor heart-lung block is carefully dissected.
For the heart recipient:
* Required cardiac structures are preserved.
* Donor valves, root, outflow tract, or partial cardiac tissue are isolated while maintaining tissue integrity.
For the lung recipient:
* Trachea is divided.
* Main pulmonary arteries and left atrial cuff are prepared.
* Bilateral lungs are separated according to institutional preference.
* Bronchial structures are prepared for implantation.
Meticulous preservation of vascular and bronchial anatomy is essential.
Implantation
Recipient 1
Partial cardiac implantation depends on the indication:
* Valve transplantation
* Root replacement
* Outflow tract reconstruction
* Partial orthotopic heart transplantation
Native myocardium may remain functional while donor tissue replaces diseased structures.
Recipient 2
Standard lung transplantation is performed:
* Bronchial anastomosis
* Pulmonary arterial anastomosis
* Left atrial cuff anastomosis
After reperfusion, ventilation is gradually restored while monitoring graft function.
Organ Preservation
Modern preservation techniques significantly improve outcomes:
* Static cold storage
* Ex vivo lung perfusion (EVLP)
* Organ Care System (OCS) for heart preservation
* Normothermic regional perfusion (NRP) in DCD donors
These technologies may extend preservation time and allow functional assessment before implantation.
Advantages
* Maximizes donor organ utilization.
* Increases the number of transplant recipients from a single donor.
* Reduces waiting-list mortality.
* Preserves viable donor tissue that would otherwise be discarded.
* Particularly valuable in pediatric transplantation, where living valve tissue can grow with the recipient.
* Supports sustainable transplantation practices.
Challenges
* Complex donor and back-table surgical preparation.
* Coordination between two independent transplant teams.
* Precise logistical planning to minimize ischemic times.
* Careful recipient matching.
* Potential ethical and allocation considerations.
Future Perspectives
Advances in normothermic machine perfusion, regenerative medicine, and partial organ transplantation are expected to expand the feasibility of multi-recipient thoracic transplantation. Living valve transplantation, partial heart transplantation in children, and sophisticated ex vivo preservation platforms may further increase donor organ utilization while improving long-term outcomes.
Conclusion
Partial heart and lung transplantation represents a significant evolution in thoracic transplantation. By allocating donor cardiac tissue to one recipient and donor lungs to another, a single donor can benefit two patients without compromising transplant quality. As surgical techniques, organ preservation, and donor management continue to advance, this strategy has the potential to become an increasingly important component of modern transplant medicine, helping address the persistent shortage of donor organs while maximizing the life-saving impact of every donation.


Dr.Sam Zeraatian Nejad Davani,
Cardiovascular and Thoracic Surgeon
Transplant and Thoracic Organs Recovery Surgeon
Director of Georgia Atlanta Procure on Demand Thoracic Organs Transplant and Procurement Surgery
S.Zeraatiannejaddavani@procureodx.com