Using echocardiography to predict fluid‑responsiveness and manage the need for fluids
Abstract
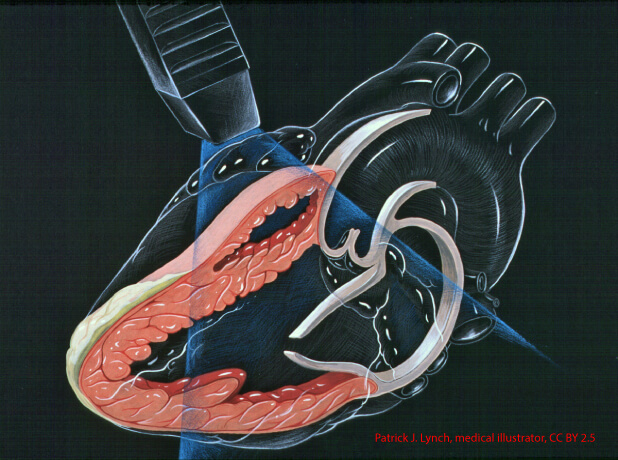
Management of fluids has progressively moved towarda more dynamic and functional approach based on theprediction of fluid responsiveness (FR), to improve effi-cacy and benefits and limit detrimental effects of fluids. Application of an optimal threshold for validatedparameters above which the patient could be fluid-responsive generates a “gray zone”. Therefore, theobjective of intensivists should be to adapt the thresholdto the respective sensitivity and specificity they need topredict FR, according to the patient’s condition. Intensiv-ists should consider being very specific in severely hypox-emic patients where fluids can be significantly harm-ful and mainly sensitive in patients without blood gasabnormalities, as maintaining non-optimal volume couldbe detrimental here. Applying a continuous approach tothe prediction of FR, i.e., how much the cardiac outputis expected to increase after fluid bolus, rather than theclassic binary one, i.e., will the patient be a “responder”,could be more efficient. Echocardiography is crucial for management ofpatients with respiratory or circulatory failure. Manyecho parameters have been proposed to predict FR.Measurement of aortic velocity time integral (VTI) iscardiac beat-related and precise enough to detect smallchanges in stroke volume, i.e., 6–4% precision whenmeasured in one or averaged in 3 cardiac beats, respec-tively, in patients in sinus rhythm with no impact of thetype of ventilation. This measurement requires a goodalignment with the ejection flow and a nice envelope withthe aortic closing sound.