High-risk pulmonary embolism: thesignificance and perspectives of pulmonaryreperfusion
Abstract
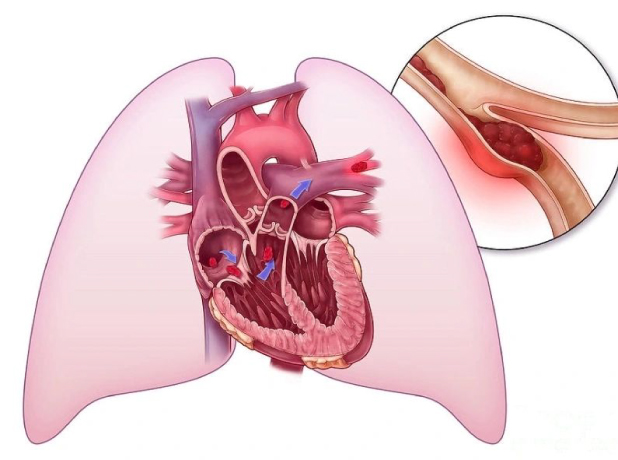
Rapid hemodynamic stabilization and restoration of pulmonary perfusion are the cornerstones of treatment for high-risk pulmonary embolism (PE). While all current guidelines recommend systemic thrombolysis (SYS) as the first-line reperfusion strategy [1, 2], other options such as surgical thrombectomy (ST) or percutaneous catheter-directed treatment (PCDT) are alternatives.
Presently, however, there is limited evidence for their first-line use in patients with high-risk PE. Mechanical cardiopulmonary support, such as veno-arterial extracorporeal membrane oxygenation (VA-ECMO), is increasingly used in high-risk PE patients with refractory shock or cardiac arrest. Yet, it remains unknown whether VA-ECMO can be used as a stand-alone technique with therapeutic anticoagulation or should only be used as a bridge to pulmonary reperfusion [3, 4]. As it is unclear which treatment option or reperfusion strategy appears superior in patients with high-risk PE, it is difficult to design and conduct randomized controlled trials.
In addition, including only patients meeting the eligibility criteria for all treatment options would require exclusion of many subjects and therefore likely introduce a selection bias into such a trial.