Theoretical Foundations of Cardiopulmonary Bypass: Bridging Science, Engineering, and Clinical Practice
Introduction: A Heart That Pauses, A Circuit That Lives
When the heart is arrested during cardiac surgery, life continues—thanks to cardiopulmonary bypass (CPB). The theoretical underpinnings of CPB stem from a deep integration of physiology, physics, and biomedical engineering. Understanding these foundations empowers perfusionists to optimize patient outcomes and make data-driven decisions in real time [1].
1. Fluid Dynamics: The Physics of Perfusion
Poiseuille’s Law:
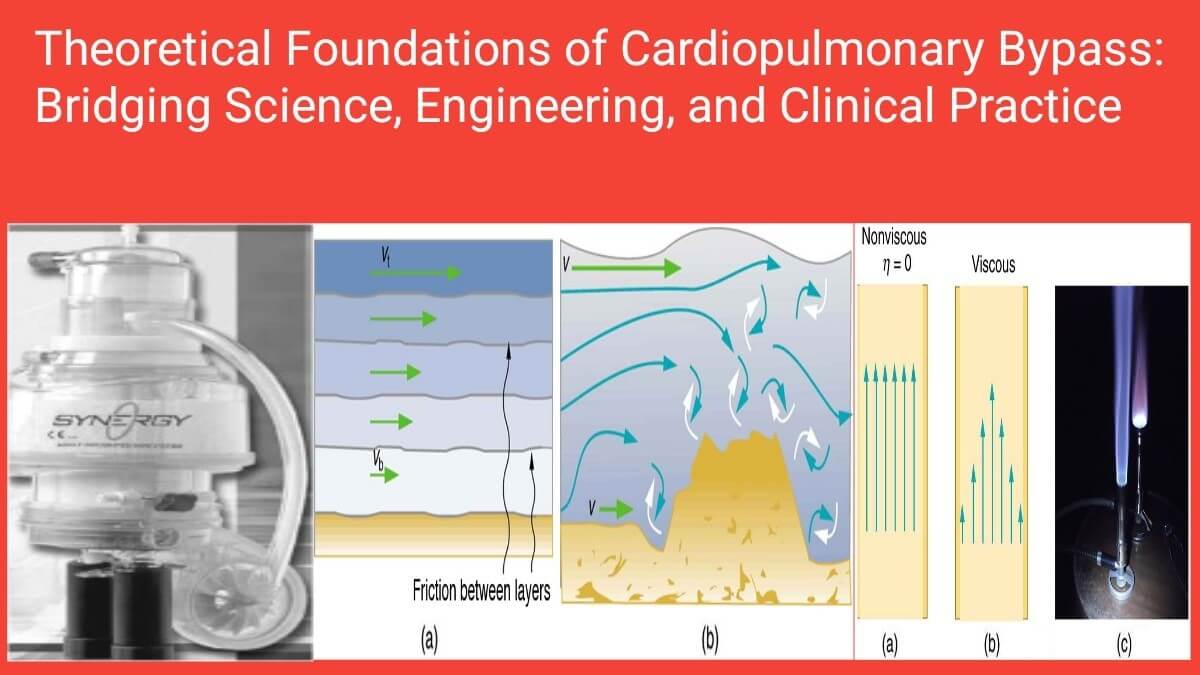
Flow through a cylindrical tube is determined by radius, viscosity, length, and pressure gradient:

This forms the basis of perfusion circuit design, highlighting why wide-bore, short tubing is preferred, and why viscosity changes due to temperature or hemodilution impact perfusion flow [2].
2. Gas Exchange: Fick’s Law and the Artificial Lung
Modern oxygenators function using Fick’s Law of Diffusion, which governs how oxygen and carbon dioxide move across semi-permeable membranes:

Optimizing membrane surface area, gas flow, and oxygen partial pressures enhances gas exchange efficiency [3]. Hollow-fiber oxygenators, with integrated heat exchangers, are designed based on this principle.
3. Thermoregulation: Cooling to Protect, Rewarming to Restore
The controlled use of hypothermia during CPB reduces metabolic demand by 6–8% per °C [4]. Fourier’s Law explains heat transfer efficiency in heat exchangers:

Overly rapid rewarming risks cerebral hyperthermia and gas bubble formation [5], which is why perfusionists follow precise gradient-limited protocols.
4. Pumps: Flow Generation with Safety Considerations
Roller Pumps:
- Positive displacement
- Flow is constant but pressure-insensitive
- Risk of excessive line pressure
Centrifugal Pumps:
- Flow varies with preload/afterload
- Reduced hemolysis
- Safer air handling
Studies have shown centrifugal pumps offer improved biocompatibility and reduce systemic inflammatory response syndrome (SIRS) during longer CPB durations [6].
5. Air Handling, Filtration & Defoaming
Arterial line filters (20–40 µm) remove microemboli and foreign debris. Reservoirs with defoamers break surface tension. Bubble detectors and circuit clamps enhance safety [7]. Together, these components prevent devastating neurologic complications like stroke and embolic injury.
6. Anticoagulation: The Balance of Clot and Flow
Unfractionated heparin remains the gold standard. The target ACT is >480 seconds, with protamine used for reversal post-bypass [8]. Advanced strategies involve antithrombin III monitoring and heparin-coated circuits for longer procedures or heparin resistance.
7. Inflammatory Response and Biocompatibility
The blood-circuit interface activates the complement cascade, leukocytes, and cytokines, contributing to SIRS. Biocompatible coatings (e.g., phosphorylcholine, PMEA) help minimize these responses [9]. Ultrafiltration and leukocyte depletion filters are valuable adjuncts, especially in pediatric cases [10].
8. Monitoring and Safety Protocols
Modern CPB circuits incorporate:
- Ultrasonic flow meters
- Pressure transducers
- Venous saturation monitoring (SvO₂)
- Air bubble detectors
- Integrated alarms and emergency shutoff systems
These measures enhance real-time safety and data-driven perfusion management [11].
9. Historical Reflection: Science that Evolved into Life Support
From John Gibbon’s successful use of the heart-lung machine in 1953 to today’s integrated consoles, CPB has evolved, but its foundational physics and physiology remain central. Mastering these principles elevates perfusion from practice to precision [12].
Conclusion: A Profession Grounded in Science
To be a perfusionist is to walk the line between engineering and healing. The theoretical underpinnings of CPB are not abstract—they’re what allow us to stop a heart and yet keep a human alive.
Let’s continue building on these foundations as we adapt to emerging challenges like ECMO, VADs, and minimally invasive perfusion.
Stay curious. Stay precise. Stay perfused.
— Asif Mushtaq Chief Perfusionist, PIC Lahore Founder – Perfusion Insight Newsletter
References
- Gravlee GP, Davis RF, Utley JR, eds. Cardiopulmonary Bypass: Principles and Practice. 3rd ed. Lippincott Williams & Wilkins; 2008.
- Poiseuille J. Recherches expérimentales sur le mouvement des liquides dans les tubes de très petits diamètres. Comptes Rendus. 1840;11:961-967.
- Fick A. On liquid diffusion. Philos Mag. 1855;10:30-39.
- Baraka AS, et al. Hypothermia and Cardiopulmonary Bypass: Clinical Applications. Middle East J Anesthesiol. 2000;15(4):407-423.
- Nathan HJ, et al. Rewarming rate and neurologic outcome after CPB. Anesth Analg. 2001;92(1):10-14.
- Bojar RM. Manual of Perioperative Care in Adult Cardiac Surgery. Wiley-Blackwell; 2021.
- Edmunds LH Jr. Inflammatory response to cardiopulmonary bypass. Ann Thorac Surg. 1998;66(5):S12–S16.
- Gravlee GP. Cardiopulmonary Bypass: Principles and Practice. 3rd Ed. Chapter on Anticoagulation.
- Asimakopoulos G, et al. Effects of heparin-bonded circuits on clinical outcome. J Thorac Cardiovasc Surg. 2000;119(2):321–329.
- Allen ML, et al. Modified ultrafiltration in pediatric cardiac surgery. Cochrane Database Syst Rev. 2010;2010(5):CD007759.
- Society of Thoracic Surgeons (STS). STS Clinical Practice Guidelines for Cardiopulmonary Bypass. Ann Thorac Surg. 2011;92(1):1–21.
- Gibbon JH. Application of a mechanical heart and lung apparatus to cardiac surgery. Minn Med. 1954;37(3):171-185.
Asif Mushtaq: Chief Perfusionist at Punjab Institute of Cardiology, Lahore, with 27 years of experience. Passionate about ECMO, perfusion education, and advancing perfusion science internationally.