Sudden severe hypotension following autologous blood transfusion: A case report
Abstract
Hypotension is a common complication during surgery that is caused by many factors.1 Among these causes, acute pulmonary air embolism is extremely rare. However, once it happens, the severe hypotension usually poses a major threat to patients.2 Here we report a severe and unusual hypotension that occurred at the end of surgery.
A 65-year-old man was referred to our hospital and diagnosed with splenic artery pseudoaneurysm and gastrointestinal bleeding. Preoperative laboratory tests revealed an acute blood loss anemia (hemoglobin level 73 g/L). Splenic artery pseudoaneurysm resection was scheduled. The surgery was completed after nearly 5 h. Intraoperative blood loss was 1 L and urine 900 mL. The patient received 8 U red blood cell suspension, 400 mL fresh frozen plasma, 1.45 L crystalloid solutions and 700 mL colloid solutions during surgery. At the end of surgery when the surgical drape was just lifted, the patient’s blood pressure plummeted to 50/40 mmHg and pulse oxygen saturation (SpO2) could not be detected. The end-tidal carbon dioxide level (EtCO2) immediately dropped from 35 to 5 mmHg and the heart rate slowed to 40 bpm.
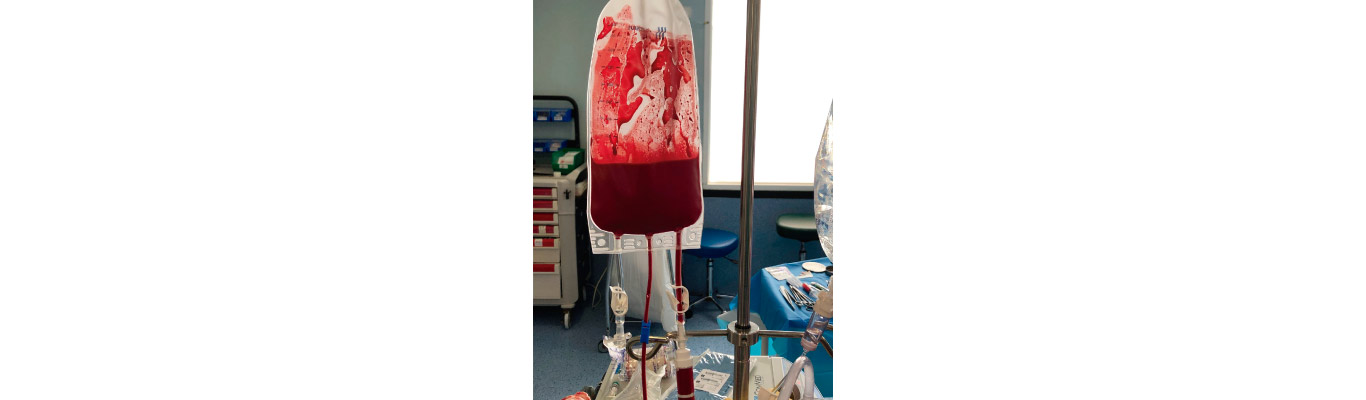
No obvious bleeding was found in the drainage tube and abdominal effusion was also not detected by B-mode ultrasound. Physical examination demonstrated slight swelling of the head and neck. These symptoms seemed to indicate that the patient had acute right heart failure. In this emergency, external chest compression was performed immediately. A total of 80 μg epinephrine and 3 mg norepinephrine and other vasoactive drugs were given in batches. The decrease in EtCO2 and SpO2 led to the conjecture that the cause was pulmonary embolism. To clarify the diagnosis, TEE was performed immediately. Right heart enlargement, intraventricular gas, and mild to moderate tricuspid regurgitation were seen (Fig. 1). The latest blood gas analysis confirmed that the partial arterial pressure of CO2 (PaCO2) was 77.8 mmHg. The paradox of PaCO2 and EtCO2, combined with the results of TEE and other signs, led to a final diagnosis of acute pulmonary air embolism. To conduct a rescue, the patient was placed in the left lateral decubitus position and air (∼20 mL) was aspirated through the internal jugular vein catheter with caution. Eventually, the patient’s condition improved significantly and EtCO2 returned to 30 mmHg. When the patient’s vital signs were stabilized, we tried to trace the source of air. It was found that the reinfusion blood bag was externally pressurized by the anesthesiologist. While there was air in the bag besides the autologous blood, the rapid infusion from the external pressurization caused air to enter the circulation. After surgery, no significant abnormalities were found. On postoperative day 6, the patient was extubated. And the patient was discharged on postoperative day 17.