Retrograde Cerebral Perfusion in Aortic Arch Surgery: Principles, Practice, and Clinical Perspectives.
1. Introduction
Cerebral protection is a cornerstone of successful aortic arch surgery, where the brain is highly vulnerable during periods of circulatory arrest. While deep hypothermic circulatory arrest (DHCA) alone was historically used, limitations in arrest time and neurologic outcomes led to the development of adjunct techniques. Among these, Retrograde Cerebral Perfusion (RCP) emerged as a means of cerebral protection, primarily through cooling, air/fluid flushing, and possibly nutritive perfusion via the venous system.
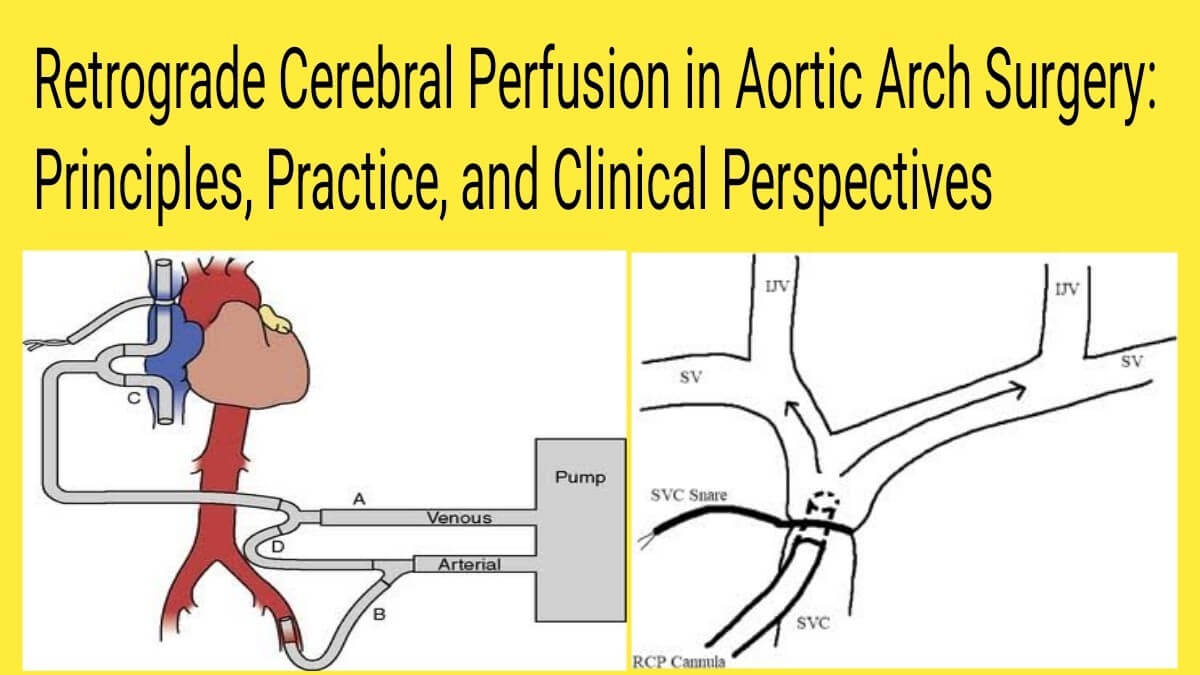
RCP delivers cold, oxygenated blood through the superior vena cava (SVC), aiming to flow in a reverse direction through the cerebral venous circulation. Though often debated, it remains a valid strategy, especially in settings where antegrade cerebral perfusion (ACP) is not available or practical. The role of RCP today is more refined and selective, rather than universal.
2. Historical Background
RCP was introduced in the late 1980s and early 1990s as an adjunct to DHCA, particularly by pioneers like Ueda and colleagues in Japan. The idea was to extend the safe ischemic time of the brain by:
- Flushing air and emboli from the cerebral vasculature
- Cooling the brain from within
- Potentially providing retrograde oxygenated blood flow to cortical structures
Initial studies suggested decreased stroke rates and improved neurologic outcomes in certain patient subsets. However, subsequent experimental models questioned whether RCP provided sufficient nutritive perfusion, especially to deeper brain regions (Urbanski et al., 2003). Nonetheless, it became an accepted strategy for brief arch repairs or emergent dissections with limited options.
3. Physiological Principles of RCP
RCP involves the infusion of oxygenated blood through the SVC under controlled pressure, with the expectation that flow travels retrograde through the jugular venous system into the brain.
Key physiological mechanisms:
- Cerebral cooling: Decreases metabolic demand
- Flush effect: Clears air and particulate emboli from cerebral arteries
- Limited perfusion: Mainly reaches cortical and superficial areas; deeper regions may not benefit
- Flow resistance: Venous valves, anatomical variability, and low pressures limit forward nutritive flow
Despite these limitations, the benefits of RCP may be more related to protection against ischemia-reperfusion injury and embolic events than true oxygen delivery.
4. Indications and Contraindications
Indications for RCP
- Emergency surgery for acute type A dissection with limited time or access for ACP
- Short-duration circulatory arrest (<30 minutes)
- Use in conjunction with DHCA for cerebral cooling and embolic protection
- Centers without facilities or experience for ACP
- Backup method if ACP fails or is not possible
- Hybrid arch repair procedures with short arrest windows
Contraindications for RCP
- Long anticipated circulatory arrest (>40 minutes)
- Preexisting SVC or jugular vein obstruction or thrombosis
- Incomplete SVC drainage pathway (e.g., persistent left SVC with bridging)
- Severe cerebral venous congestion or intracranial hypertension
- Lack of monitoring capability for cerebral saturation or perfusion pressure
- Cases requiring full-body perfusion during arrest
5. Techniques and Perfusion Parameters
Cannulation
- Site: Superior vena cava or innominate vein
- Snares applied to isolate cerebral venous return
- Atrial drainage from IVC continues separately
Perfusion Parameters
Parameter Target Range Flow Rate 300–500 mL/min Perfusion Pressure 15–25 mmHg Temperature 12–18°C (deep hypothermia) Duration Ideally <30 minutes
Monitoring
- EEG: Suppression indicates adequate cooling
- NIRS (Near-Infrared Spectroscopy): Monitors rSO₂; less reliable with venous route
- Jugular bulb temperature and pressure: Helps ensure safe and effective retrograde flow
6. Clinical Outcomes and Evidence
While RCP is inferior to ACP in providing nutritive cerebral perfusion, it does offer measurable benefits:
- Reduced stroke risk compared to DHCA alone
- Lower embolic load in experimental models
- Adequate protection for short arrest times
A meta-analysis by Tian et al. (2015) comparing RCP and ACP concluded:
- RCP may reduce stroke risk compared to DHCA alone
- ACP remains superior for longer, complex repairs
Modern centers rarely rely on RCP as a standalone strategy for prolonged arch procedures, but it is still useful in specific clinical scenarios.
7. Current Controversies
- Effectiveness as nutritive perfusion: Some argue RCP is not truly perfusing cerebral tissue beyond superficial zones.
- Monitoring reliability: Conventional tools like NIRS and EEG may not accurately reflect perfusion in RCP.
- Air flushing vs oxygen delivery: Debate remains whether its benefit lies more in preventing emboli than feeding the brain.
- Standardization: Techniques, flow rates, and pressures vary significantly between institutions.
8. Evolving Role and Future Perspectives
Although ACP has become dominant in modern aortic arch surgery, RCP remains valuable in selected cases. Future directions include:
- Selective use in hybrid and minimally invasive arch repair
- Combining RCP with pharmacologic brain protection (e.g., magnesium sulfate, steroids)
- Real-time SVC flow-guided systems to optimize perfusion without overpressure
- Smart perfusion integration: AI-based feedback to auto-adjust retrograde flow and pressure
Ultimately, RCP may evolve into a complementary technique, used in conjunction with ACP or DHCA, tailored to individual anatomy and surgical complexity.
9. Conclusion
Retrograde cerebral perfusion, once considered a breakthrough in cerebral protection, now plays a more targeted role in modern aortic surgery. Its benefits include cerebral cooling, embolic protection, and limited superficial perfusion during short arrest. While not a replacement for ACP in complex or prolonged procedures, it remains a useful tool in specific emergencies and selected patients. The future of cerebral protection lies in patient-specific, multimodal, and monitored strategies — with RCP remaining part of the perfusionist’s toolkit.
Asif Mushtaq: Chief Perfusionist at Punjab Institute of Cardiology, Lahore, with 27 years of experience. Passionate about ECMO, perfusion education, and advancing perfusion science internationally.