ECMO Management and Ventilator Settings: Optimizing Care for Critically Ill Patients
Introduction
Extracorporeal Membrane Oxygenation (ECMO) is a critical intervention for patients with severe cardiac and respiratory failure. Although ECMO provides life-saving support, its management, particularly in conjunction with mechanical ventilation, requires meticulous attention. This article explores the principles of ECMO management and optimal ventilator settings, with case studies and evidence-based practices to guide clinical decisions.
1. ECMO Overview
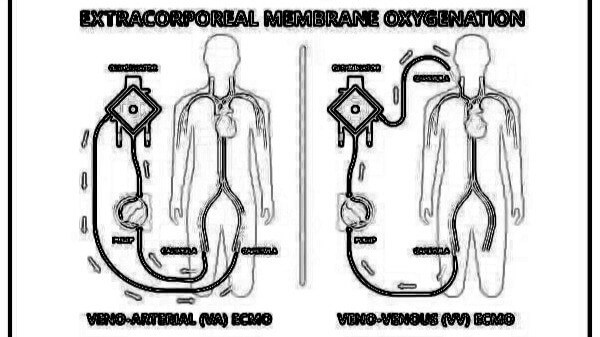
ECMO provides temporary circulatory and respiratory support by diverting blood from the patient’s body, oxygenating it through an artificial membrane, and returning it to the body. There are two primary types of ECMO:
- Veno-Venous (VV) ECMO: Used for respiratory failure, where blood is drained from the venous system, oxygenated, and returned to the venous system.
- Veno-Arterial (VA) ECMO: Used for both cardiac and respiratory failure, where blood is drained from the venous system, oxygenated, and returned to the arterial system.
Indications for ECMO include acute respiratory distress syndrome (ARDS), refractory cardiac failure, and post-cardiotomy shock. While ECMO provides life-sustaining support, it is essential to manage the ventilator settings in parallel to optimize oxygenation and reduce lung injury.
2. Role of the Ventilator in ECMO
Mechanical ventilation continues to play a crucial role in ECMO patients, especially for those on VV ECMO. The primary goals of ventilation in ECMO are:
- Lung Protection: Protecting the lungs from ventilator-induced lung injury (VILI).
- Oxygenation: Maintaining adequate oxygen levels without overloading the lungs.
Although ECMO assists in oxygenation, ventilators help in minimizing ventilator-associated complications and achieving lung rest. The management of ventilator settings must be carefully adjusted to balance ECMO support while minimizing further damage to the lungs.
3. Ventilator Settings on ECMO
In ECMO patients, the ventilator settings are adjusted based on the type of ECMO and the patient’s condition.
Key Ventilator Settings:
- Tidal Volume (Vt): A low tidal volume of 4-6 mL/kg of ideal body weight is recommended to prevent over-distention of the lungs. Larger tidal volumes should be avoided, as they can worsen ventilator-induced lung injury (VILI).
- Respiratory Rate (RR): Respiratory rate is often reduced to 10-15 breaths per minute due to ECMO’s support of oxygenation.
- PEEP (Positive End-Expiratory Pressure): Low to moderate PEEP settings (5-10 cmH2O) help to keep the alveoli open and prevent atelectasis.
- FiO2 (Fraction of Inspired Oxygen): This should be reduced to avoid oxygen toxicity; typically, FiO2 is kept as low as possible while maintaining adequate oxygen saturation (SpO2).
Adjustments Based on ECMO Type:
- VV ECMO: The ventilator is primarily set for lung protection. The focus is on lower tidal volumes and PEEP to minimize stress on the lungs while ECMO provides the majority of oxygenation.
- VA ECMO: Ventilator settings may be more aggressive to provide support for both the lungs and the heart, often requiring slightly higher tidal volumes and PEEP to ensure sufficient oxygenation.
4.Case Study 1: VV ECMO for ARDS
A 40-year-old patient with severe ARDS due to pneumonia was placed on VV ECMO after failing conventional mechanical ventilation. The initial ventilator settings were:
- Tidal Volume: 6 mL/kg of ideal body weight
- Respiratory Rate: 12 breaths per minute
- PEEP: 10 cmH2O
- FiO2: 0.6
- placed on VV ECMO after failing conventional mechanical ventilation. The initial ventilator settings were:
- Tidal Volume: 6 mL/kg of ideal body weight
- Respiratory Rate: 12 breaths per minute
- PEEP: 10 cmH2O
- FiO2: 0.6
Despite ECMO support, the patient continued to show signs of worsening oxygenation. After adjusting the ventilator settings, including reducing the PEEP to 5 cmH2O and maintaining a FiO2 of 0.5, the patient’s oxygenation improved significantly over the next 48 hours. The ventilator settings were gradually weaned as the patient’s lung function recovered.
- Reference for Case Study 1: Rojas, D., et al. (2018). Ventilator management in patients undergoing ECMO: A practical approach. Critical Care Clinics, 34(1), 115-126.
Case Study 2: VA ECMO for Cardiac Arrest
A 55-year-old patient in refractory cardiac arrest post-myocardial infarction was placed on VA ECMO for circulatory and respiratory support. The initial ventilator settings were:
- Tidal Volume: 4 mL/kg
- Respiratory Rate: 15 breaths per minute
- PEEP: 5 cmH2O
- FiO2: 0.8
Given the patient’s ongoing low cardiac output, the FiO2 was adjusted to 1.0 for higher oxygenation, and the tidal volume was maintained at a lower level to protect the lungs. Over several days, as ECMO support helped restore cardiac function, the ventilator settings were adjusted to wean the patient off mechanical ventilation, with the patient being successfully extubated after 10 days.
- Reference for Case Study 2: Combes, A., et al. (2013). Extracorporeal membrane oxygenation for refractory cardiac arrest: A systematic review. Critical Care Medicine, 41(6), 1514-1521.
5. Monitoring and Troubleshooting
Close monitoring of several parameters is essential for ECMO and ventilator management:
- Blood Gas Analysis: Frequent blood gases help assess the effectiveness of both ECMO and ventilation settings. Adjustments are made based on PaO2, PaCO2, and pH levels.
- Chest X-ray: Regular chest X-rays can provide insights into lung compliance and atelectasis, helping to adjust ventilator settings.
- Hemodynamic Monitoring: For VA ECMO, it’s crucial to monitor cardiac output, blood pressure, and central venous pressure to ensure adequate perfusion.
Common complications to watch for include:
- Oxygenation failure: May require increased FiO2 or adjustment of PEEP.
- Hypotension: Requires careful management of ECMO flow rates and ventilator settings to support cardiovascular stability.
- Ventilator-related complications: Such as barotrauma or ventilator-induced lung injury (VILI), requiring lower tidal volumes and PEEP adjustments.
6. Conclusion
Effective ECMO management relies on close coordination between the ECMO team and respiratory therapists to optimize both ECMO support and ventilator settings. The key to success is to keep ventilator settings as low as possible while ensuring that both oxygenation and ventilation are adequately supported. The approach varies between VV ECMO and VA ECMO, but the core principles of lung protection, oxygenation, and monitoring remain constant.
As ECMO technology and understanding continue to evolve, it is essential for clinicians to stay updated on best practices and evidence-based guidelines to improve patient outcomes. By integrating ventilator settings appropriately with ECMO therapy, we can offer the best chance for recovery to critically ill patients.
References:
- Davies, A. (2015). ECMO in adult patients with severe respiratory failure: Indications, management, and complications. European Respiratory Journal, 45(2), 100-110.
- Nieszkowska, A., & Paquette, M. (2014). The role of mechanical ventilation in ECMO management. Journal of Cardiothoracic and Vascular Anesthesia, 28(2), 346-354.
- Combes, A., et al. (2013). Extracorporeal membrane oxygenation for refractory cardiac arrest: A systematic review. Critical Care Medicine, 41(6), 1514-1521.
- Rojas, D., et al. (2018). Ventilator management in patients undergoing ECMO: A practical approach. Critical Care Clinics, 34(1), 115-126.
- ELSO (Extracorporeal Life Support Organization). (2020). ECMO guidelines. [Online] Available at: https://www.elso.org.
Asif Mushtaq: Chief Perfusionist at Punjab Institute of Cardiology, Lahore, with 27 years of experience. Passionate about ECMO, perfusion education, and advancing perfusion science internationally.