Antegrade Cerebral Perfusion in Aortic Surgery: Techniques, Evidence, and Future Perspectives.
1. Introduction
Aortic arch surgery presents significant neurologic risks due to the potential for cerebral ischemia during circulatory arrest. Traditional methods such as deep hypothermic circulatory arrest (DHCA) provided limited time for safe surgical intervention but were associated with high stroke rates, neurocognitive decline, and mortality. In recent decades, Antegrade Cerebral Perfusion (ACP) has emerged as a cornerstone technique for cerebral protection during complex aortic procedures. By supplying oxygenated blood in a physiologic, forward direction through the carotid and vertebral arteries, ACP allows for extended operative time, improved neurologic outcomes, and greater procedural safety (Bavaria et al., 2015; Di Eusanio et al., 2013).
2. Historical Background
Neuroprotection strategies have evolved significantly over the last 60 years. Initial reliance on DHCA alone allowed for brief safe periods of circulatory arrest, with brain cooling suppressing cerebral metabolism. However, complications remained high for prolonged arrests (>30 minutes) (Kazui et al., 1996). This led to the development of Retrograde Cerebral Perfusion (RCP), which aimed to provide cerebral blood flow via the superior vena cava in a reverse direction. Despite early interest, RCP failed to consistently deliver adequate perfusion, especially to deeper brain structures (Urbanski et al., 2003).
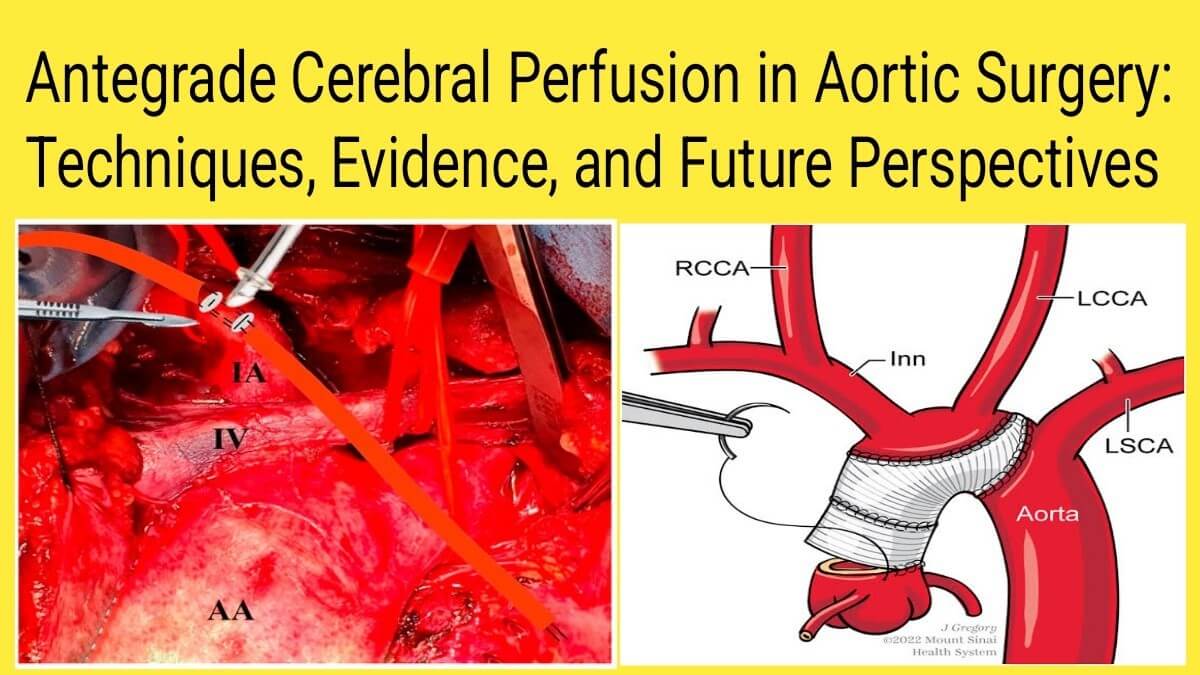
In the 1990s, ACP emerged as a superior alternative. First introduced by Bachet and Kazui, ACP allowed for direct, physiological perfusion of the brain via the arterial system, either unilaterally (via the right axillary or innominate artery) or bilaterally (by also perfusing the left carotid artery) (Bachet et al., 1991; Kazui et al., 1992). This innovation significantly reduced neurologic complications, expanding the surgical envelope for aortic arch interventions.
3. Techniques of ACP
3.1 Cannulation Strategies
- Unilateral ACP involves cannulation of the right axillary or innominate artery, relying on the Circle of Willis to distribute flow bilaterally.
- Bilateral ACP adds direct perfusion to the left common carotid artery, used when the circle is incomplete or in prolonged procedures.
3.2 Perfusion Parameters
- Flow Rate: 10–15 mL/kg/min
- Pressure: 40–70 mmHg
- Temperature: Typically 22–26°C (moderate hypothermia)
3.3 Monitoring
- Near-infrared spectroscopy (NIRS) monitors regional cerebral oxygen saturation.
- Transcranial Doppler (TCD) evaluates blood flow velocity in cerebral arteries.
- Electroencephalography (EEG) tracks electrical brain activity and depth of anesthesia.
These tools help tailor perfusion parameters in real-time and detect potential malperfusion early.
4. Clinical Outcomes and Evidence
Numerous studies have shown that ACP, especially when combined with moderate hypothermia, leads to significantly better outcomes compared to DHCA or RCP. Stroke rates with ACP are typically below 5%, even in complex aortic reconstructions (Di Eusanio et al., 2013). A meta-analysis by Tian et al. (2015) found ACP associated with reduced mortality and neurologic injury compared to RCP.
Furthermore, unilateral ACP is safe in the majority of patients, though bilateral ACP may be preferred in cases with incomplete circle of Willis or prolonged circulatory arrest (>40 minutes) (Preventza et al., 2020).
5. Controversies and Considerations
While ACP is widely accepted, key debates persist:
- Unilateral vs Bilateral ACP: Evidence supports both approaches, but bilateral perfusion may provide superior protection in patients with anatomical variations or longer procedures.
- Perfusion Flow and Pressure: Overperfusion can cause cerebral edema, while underperfusion risks ischemia. Hence, individualized monitoring is essential.
- Temperature Management: There’s a trend toward using moderate hypothermia (24–28°C) instead of deep hypothermia (<20°C), reducing the risk of coagulopathy and allowing faster postoperative recovery (Di Eusanio et al., 2013).
6. Recent Advances
Recent years have seen several innovations:
- Hybrid aortic arch procedures combining open and endovascular techniques often incorporate ACP.
- Mild hypothermia ACP protocols are being investigated to shorten cooling and rewarming time.
- Smart perfusion systems, integrating real-time data from NIRS and pressure sensors, aim to adjust cerebral flow dynamically.
- Axillary cannulation has become standard in many centers, offering safe access and reduced embolic risk.
7. Future Directions
Future strategies aim to further enhance cerebral safety through:
- Artificial intelligence (AI) for automated perfusion control and early detection of malperfusion.
- Neuroprotective pharmacologic agents, such as adenosine or magnesium, to reduce ischemic injury.
- Biomarkers like S100β and neuron-specific enolase (NSE) to detect subclinical brain injury.
- 3D perfusion mapping using imaging data to guide cannulation and predict risk zones.
These advancements, combined with a better understanding of cerebrovascular anatomy and individualized perfusion targets, will continue to improve outcomes in aortic surgery.
8. Conclusion
Antegrade cerebral perfusion has transformed the landscape of aortic arch surgery, offering superior neurologic protection and enabling safer, more complex operations. Through refinement of cannulation techniques, optimal perfusion parameters, and advanced monitoring, ACP now serves as a standard of care in many centers. Ongoing research into AI-driven perfusion control, tailored temperature strategies, and intraoperative biomarkers promises to further enhance cerebral outcomes and precision in the field of cardiac surgery.
Asif Mushtaq: Chief Perfusionist at Punjab Institute of Cardiology, Lahore, with 27 years of experience. Passionate about ECMO, perfusion education, and advancing perfusion science internationally.