Cor pulmonale

🎥1️⃣: Note how skewed this PLAX view is with the LV compressed by a massively dilated RV. Typically only the RVOT is seen in this view not most of the RV.
🎥2️⃣: PSAX sows septal motion consistent with pressure and volume overload. The left ventricle is classically D shaped, which is best seen throughout all of diastole (hence volume overload). In systole, when the LV contracts the septum tries to allow the LV to approximate more of a circular shape, but not fully, suggestive some pressure overload as well. A pericardial effusion is also present, which is not uncommon in CP.
{kind=link}
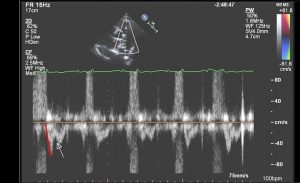
📷3️⃣: This pulsed wave Doppler shows several important features consistent with PHT. First the RVOT VTI is notched (white arrow), quite abnormal due to reflected waves that return during RV systole. Also note the steep acceleration time to peak velocity (red line), 60ms in this individual (<80ms in this context goes along with high PA pressures).
🎥4️⃣: This apical 4 chamber shows the right ventricle is severely enlarged and hypertrophied. It is also apex forming (meaning that the majority of the ventricular apex is made up by the RV and not LV). The RA is also markedly dilated with the inter-atrial septum bowed into the LA due to elevated right sided pressures.
🎥5️⃣: The tricuspid annulus is dilated, the leaflets barely coapt, and significant tricuspid regurgitation (TR) is present.

{kind=link}
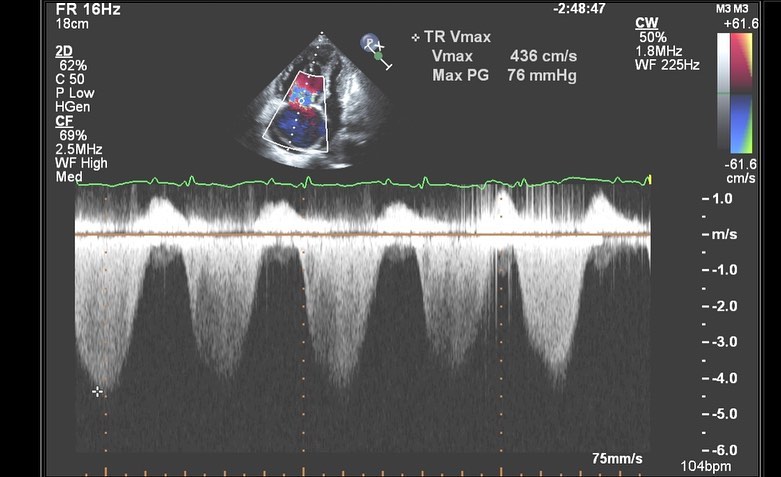
📷6️⃣: CW Doppler shows a thick dense TR jet. The estimated PA systolic pressure is markedly elevated. Adding on an RA pressure of 15, which this individual had, yields a PA systolic pressure of nearly 90 mmHg.
From echocardiographer.org